
Transkript
FOKUS BRONCHIALKARZINOM
Early stage Non-Small Cell Lung Cancer – Comparison of surgery and stereotactic body radiotherapy
Surgery is the standard of care for operable patients with early stage lung cancer. Yet, it is not always possible, as many patients are elderly, have comorbidities or may refuse to undergo an operation. For many of these situations stereotactic body radiotherapy (SBRT) is a good alternative. In this article we want to address diagnostics, staging, prognosis and therapeutic options of early stage lung cancer and want to compare surgery and SBRT.
FABIO DENNSTÄDT, PAUL MARTIN PUTORA, PAWEL LESKOW
SZO 2022; 5: 6–10
Dr. med. Fabio Dennstädt Prof. Dr. Paul Martin Putora Dr. Pawel Leskow
Epidemiology
With about 3300 deaths each year, lung cancer is the most frequent cause of cancer-related deaths in Switzerland (1). Lung cancer mostly affects the elderly with a median age of around 70 years at time of diagnosis (2), and many of them have comorbidities or a reduced performance status. Although tobacco consumption in industrial nations has declined over the last decades, smoking (actively as well as passively) remains the most important risk factor.
Symptoms and diagnosis
The most common symptoms of lung cancer are cough, pain, dyspnoea, haemoptysis and weight loss, which all occur predominantly in more advanced tumors (3). The diagnostic tests used in the initial evaluation of patients presenting with symptoms suspicious for lung cancer include clinical examination, lab tests, chest X-ray, CT thorax and bronchoscopy with biopsy (including mediastinal staging) (4). Further diagnostic procedures for staging the tumor may involve FDG-PET/CT, puncture of pleura or effusion, imaging of the head (ideally
ABSTRACT
Surgery is the standard of care for operable patients with early stage lung cancer. Yet, it is not always possible, as many patients are elderly, have comorbidities or may refuse to undergo an operation. For many of these situations stereotactic body radiotherapy (SBRT) is a good alternative. In this article we want to address diagnostics, staging, prognosis and therapeutic options of early stage lung cancer and want to compare surgery and SBRT.
Keywords: Non-Small Cell Lung Cancer (NSCLC), video-assisted thoracoscopy (VATS), robot-assisted thoracoscopic surgery (RATS), stereotactic body radiotherapy (SBRT)
with an MRI), mediastinoscopy or video-assisted thoracoscopy (VATS).
Early Stage Lung Cancer
Lung cancer in general can be staged according to the TNM classification (5). Early stage lung cancer (Stage I-IIA) corresponds to a situation of limited localized tumor growth without affection of lymph nodes (Table).
Histologically, lung cancer can be classified as Non-Small Cell Lung Cancers (NSCLC) or SmallCell Lung Cancers (SCLC), which has major implications on treatment and prognosis of the disease. The majority (85%) of lung cancer cases are NSCLC, which are themselves a heterogeneous group, that may be further divided into adenocarcinoma, squamous cell carcinoma and large cell carcinoma (7, 8). Yet, histological sampling may not always be possible (e.g. due to location or comorbidities). Most cases of lung cancer are diagnosed in an advanced tumor stage and only in a minority of cases lung cancer is still in an early stage (8.3% stage I and 7.3% stage II) (3). Many patients with early stage lung cancer do not have any symptoms at the time of diagnosis. As a result, early stage lung cancer is often an incidental finding, with a suspicious lesion being seen on CT scan or chest x-ray (9). While some lesions may present with typical radiological signs of malignancy, others may appear as non-solid nodules, called ground glass opacities (GGO). Overall, cases of lung cancer are often highly individual oncological situations. The peculiarities of
6 SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 5/2022
FOKUS BRONCHIALKARZINOM
Table
T1 stadium
T1 diameter ≤ 3cm T1a(mi) minimal invasive adenocarcinoma T1a diameter ≤ 1 cm T1b diameter > 1 and ≤ 2 cm T1c diameter > 2 and ≤ 3 cm T2 diameter > 3 and ≤ 5 cm and/or
• infiltration of main bronchus or • infiltration of visceral pleura or • obstruction leading to atelectasis or pneumonia T2a diameter > 3 and ≤ 4 cm T2b diameter > 4 and ≤ 5 cm UICC-8 tumor stage
IA T1a(mi), T1a IA2 T1b IA3 T1c IB T2a IIA T2b
T stadium and UICC-8 stage of early stage, nodal negative lung cancer (adapted from [6]).
an individual case, including patient history and comorbidities, as well as social aspects need to be considered. The oncological situation and therapeutic options should be discussed within interdisciplinary tumor boards and in a shared decisionmaking with the patient.
Surgery
Evaluation of operability In general, the standard treatment of early stage NSCLC is a surgical approach, as recommended by international guidelines such as the German S3 guideline (10) or the guideline of the National Comprehensive Cancer Network (11). To perform surgery, the clinical as well as the functional operability of the patient must be warranted (12). A cardiopulmonary assessment, involving functional diagnostic using spirometry and/or spiroergometry, as well as potentially other cardiological or pulmonary examinations are required to estimate the operability.
Therapeutic procedure In patients with sufficient pulmonary reserve a lobectomy with mediastinal lymphadenectomy is the most commonly recommended treatment. Many of these resections are performed minimalinvasively (video-assisted thoracoscopy [VATS] or robot-assisted thoracoscopic surgery [RATS]) due
to the small tumor size and absence of mediastinal lymphadenopathy. However, there is an ongoing debate on how to proceed in cases of peripheral pure GGO, which might be malignant in over half of cases (13, 14). The question of whether a pure GGO needs the same oncological resection as a solid growing cT1c, cN0 NSCLC remains unanswered (15). A sublobar resection is considered an acceptable surgical option for pure GGO lesions or adenocarcinoma in situ (16). A standard lobectomy with mediastinal lymphadenectomy in early stage NSCLC is performed in an open surgery – via thoracotomy, or minimal-invasively via VATS/RATS. The decision is made by the surgeon depending on tumor localization, tumor size, surgeon’s expertise, comorbidities, etc. As there are no significant differences in nodal upstaging, 30-day mortality and 5-year survival (17), the resection should be performed minimal-invasively due to a shorter length of stay and less postoperative pain (18). Independently of the resection modality, mediastinal lymphadenectomy leads to more accurate oncological therapy, because in 5–15% of the cases, there is an unforeseen pathological N2 involvement which may require adjuvant therapy (19). A different situation is present in patients unable to undergo a lobectomy due to poor pulmonary function. There are other surgical resection modalities apart from lobectomy which may be considered. If the tumor is located peripherally within the lobe or can be assigned to a specific pulmonary segment, segmentectomy or wedge resection can be considered. The advantage of segmentectomy is the possibility of harvesting the N1 lymph nodes in the intersegmental plane which is not possible in wedge resections. As studies comparing the oncological outcomes between lobectomies and segmentectomies for stage IA adenocarcinoma showed no inferiority of less extensive resection procedures, they present a surgical treatment option for patients with limited pulmonary function (20, 21). Sublobar resection may be considered in synchronous or metachronous primary lung cancer.
Possible complications and side effects Postoperative morbidity after pulmonary resection is not rare. The internationally known rate for mortality after lobectomy is 2.6% and the rate for morbidity is 10–15%. The risk for postoperative complications rises with patients age (22). A common complication after a pulmonary resection is a prolonged air leak, defined as a leak lasting more than 7 days (22). As most of the NSCLC patients undergoing treatment are former/current smokers, the incidence of lung emphysema is high. Therefore, attention should be paid to avoid damaging
SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 5/2022
7
FOKUS BRONCHIALKARZINOM
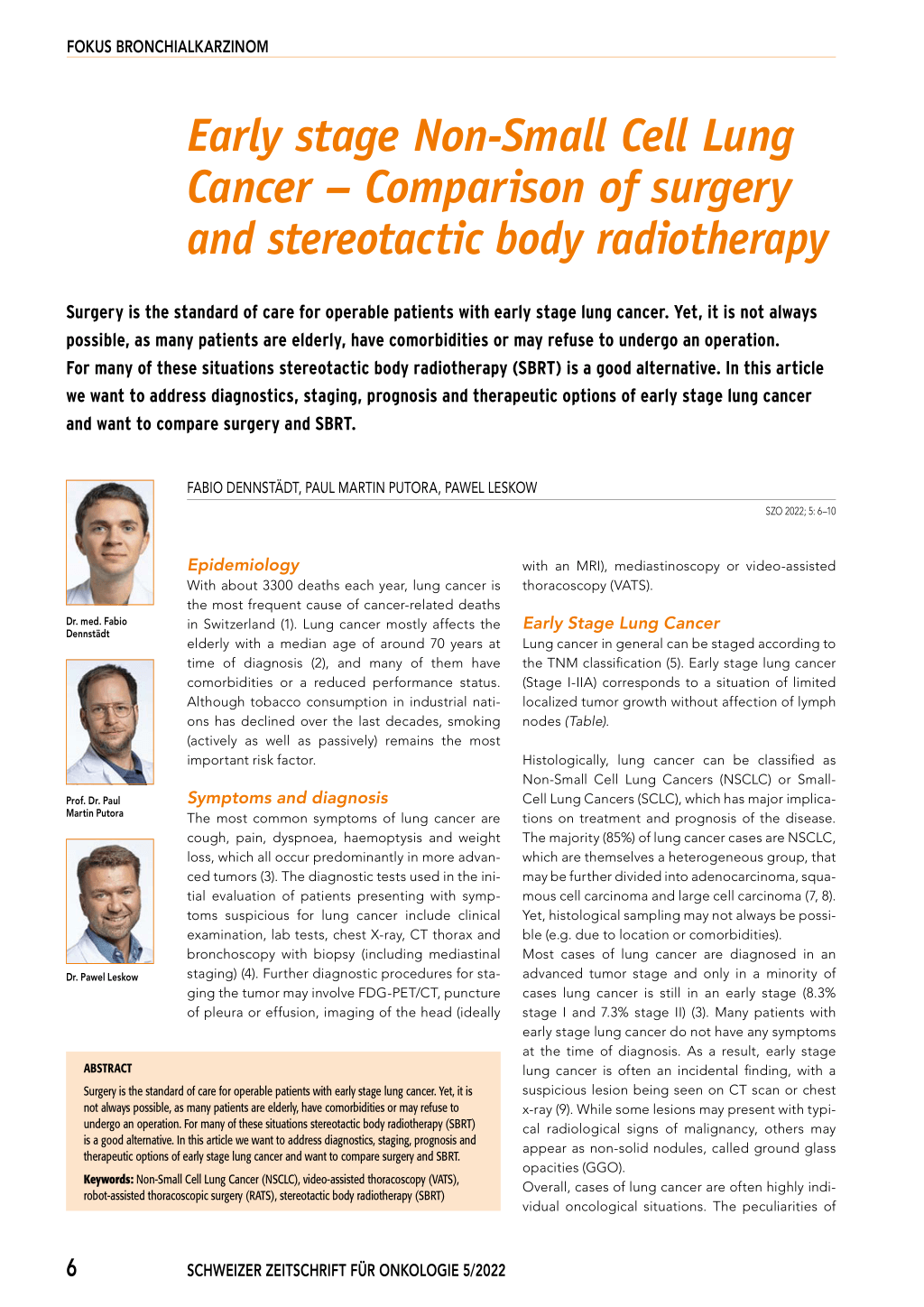
Figure 1: Image of a linear accelerator and of the dose profile of an SBRT
tumor-free lung parenchyma. Postoperative extubation should be assessed as soon as possible. One of the common complications following pulmonary resection, especially in elderly, is atrial fibrillation with an incidence of about 30% (23). Specific complications for pulmonary resection include: nerve injury, chylothorax, pneumonia, empyema, atelectasis, bronchopleural fistula.
Prognosis In selected patients eligible for sublobar resec tions, some studies reported similar survival rates between lobectomy and segmentectomy. In a latest study comparing 1018 patients with N0 invasive lung adenocarcinomas smaller than 2 cm, after propensity-score matching, no significant difference of overall survival or recurrence-free survival was found (24). 5-year survival rates have been shown to be 67% for stage IA and 55% for stage IIA (25).
Stereotactic Radiotherapy
Preparation of a radiotherapy As mentioned before, patients with lung cancer are often elderly and may have comorbidities and an impaired general health state. For patients who are inoperable or who do not want to undergo surgery, stereotactic body radiotherapy (SBRT) is a good therapeutic alternative with curative intention (25). Often a pulmonary assessment is performed before therapy to estimate the risk of side effects.
Planning CT In order to perform a radiotherapy, a planning CT needs to be done. As the application of radiation is precisely calculated in modern 3D-conformal radiotherapy, the planning CT is required as a reference image, on which the calculations are done. Correct positioning of the patient needs to be ensured and in the case of lung cancer, the movement of the tumor during the breathing needs to be evaluated. In some situations, further aspects may be considered, such as application of certain breathing techniques.
Determination of radiation volume and dose After the planning CT, the radiation oncologists define the target volume as well as organs at risk, which need to be considered for the radiation treatment plan. In the case of SBRT, the defined volume that is planned to receive a high radiation dose is relatively small, including the tumor and only a narrow safety margin around it. Regarding radiation dose, «stereotactic» or hypofractionated dose regimes (> 2 Gy per fraction) are usually used for SBRT of early stage lung cancer. While normofractionated schemes of 2 Gy per fraction are used in many radiooncological situations and also are common in more advanced stages of lung cancer, for early stage NSCLC hypofractionated SBRT has shown better results (27). As a result, SBRT is today the standard of care for patients with medically inoperable early stage NSCLC (Figure 1) (28).
Commonly used treatment regimens usually comprise three to eight fractions with a biologically equivalent dose of more than 100 Gy, as it has been shown that these higher doses lead to higher rates of local control (29, 30). Commonly used regimes include schemes of 3 x 13.5 Gy, 3 x 18 Gy, 5 x 11 Gy or 8 x 7.5 Gy (29).
Possible complications and side effects A common side effect of radiation therapy is tiredness. More serious side effects of SBRT, especially if the tumor is close to critical structures, involve chest wall pain, rib fracture, esophagitis or brachial plexopathy (31). Another rare, but serious potential side effect of SBRT is the development of a severe radiation pneumonitis, which may lead to coughing, dyspnoea, fever and pleuritic pain and may require a corticosteroid therapy. In a meta-analysis of multiple observational studies the rate of severe (≥ grade 3) radiation pneumonitis after SBRT was 2% (32).
Prognosis Numerous studies have shown that SBRT is an effective treatment to ensure ablation of radiated
8 SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 5/2022
FOKUS BRONCHIALKARZINOM
tumor sites with 3-year local control rates of around 90% (25). In a study of Timmerman et al. rates of 3-year survival were 55.8% (with a median survival of 48.1 months) for patients with early stage NSCLC treated with SBRT (26).
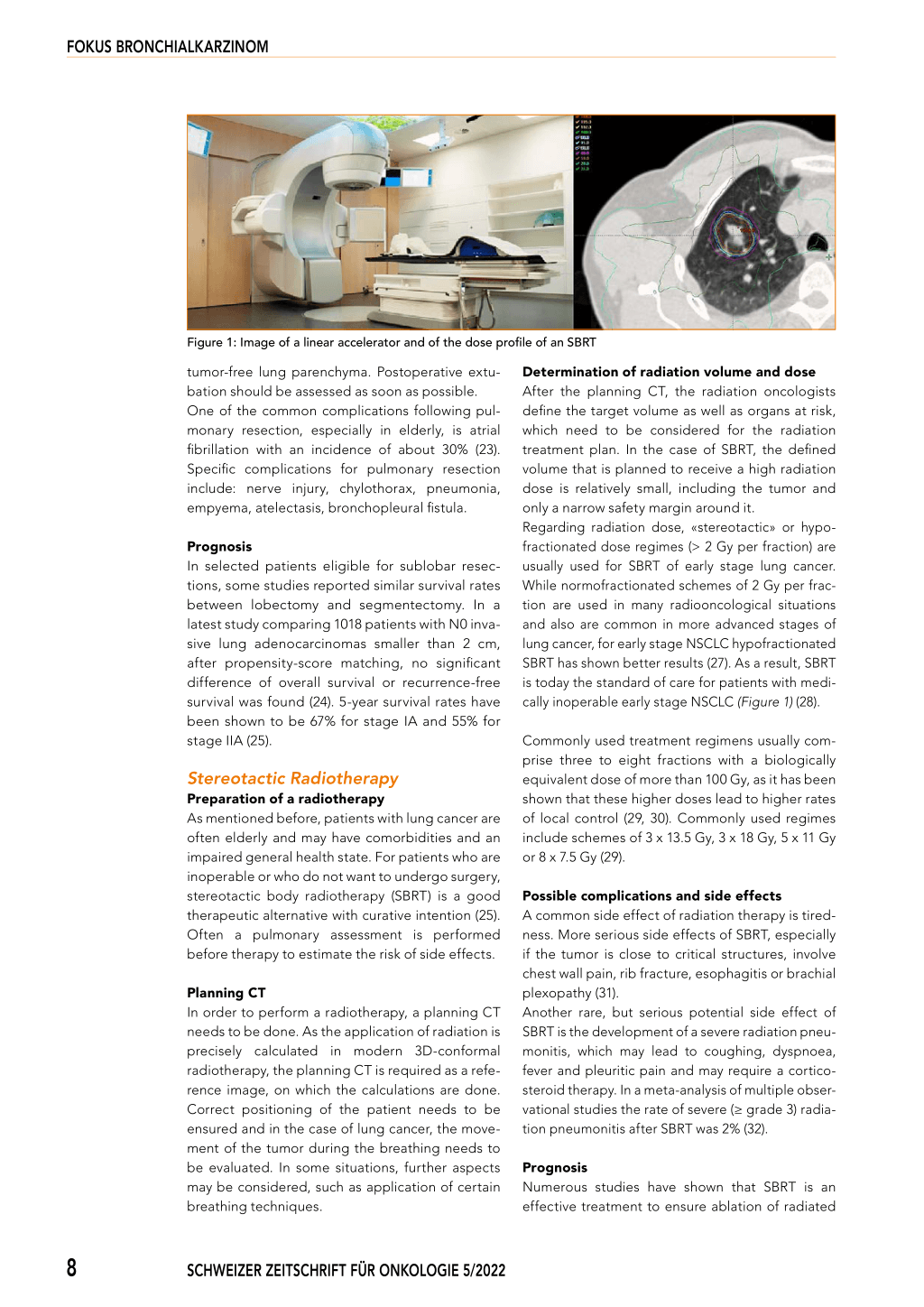
Comparison of surgery and SBRT (Conclusion) Attempts to directly compare surgery and SBRT in stage I NSCLC were undergone in the STARS (33) and in the ROSEL trial (34). Unfortunately, both trials were closed early due to low patient recruitment. In a pooled analysis, the estimated rates of overall survival at 3 years were 86% for SBRT and 80% for surgery (35). Yet, the data are not sufficient to prove equivalence of SBRT to surgery. In a retrospective analysis that compared lobectomy and SBRT for stage I/II NSCLC, 3-year survival rates were in favor of surgery with 92.8% over 59% (36). In a propensity matched comparative Dutch analysis from 2019, 792 patients aged > 65 years with NSCLC stage I underwent VATS lobectomy or SBRT. In matched groups the 1-, 3- and 5-year OS rates after VATS lobectomy were 91%, 68% and 58% and 87%, 46% and 29% after SBRT (p < 0.001). The survival advantage with VATS lobectomy also persisted after adjusting for non-matched variables (p = 0.034) (37). Figure 2: Comparison of surgery and SBRT for early stage lung cancer Overall, surgery remains the standard of care for medically operable patients as stated by international guidelines (10, 11). Beyond mere outcome, surgery also facilitates histological examination of the tumor, which may be helpful in situations where histological testing is needed. Furthermore, if a hilar or mediastinal lymphadenectomy is performed, this may lead to tumor upstaging and require further adjuvant therapy. FOKUS BRONCHIALKARZINOM Key points ■ Patients with early stage lung cancer often do not have any symptoms ■ Diagnostic procedures involve clinical examination, lab tests, imaging techniques and bronchoscopy with biopsy and mediastinal staging ■ A cardiopulmonary examination is required to check for functional operability (if an operation is considered) ■ Surgery is the standard of care for operable patients in early stage NSCLC ■ SBRT is a good alternative with high rates of local control for inoperable patients and patients refusing to undergo surgery In general, surgery and SBRT differ in terms of treatment procedure. While an operation necessitates hospitaliziation and narcosis of the patient, the SBRT requires several visits, usually daily for two weeks (Figure 2). While surgery is the current standard of care for early stage lung cancer, SBRT is a good therapeutic option for inoperable patients or patients refusing surgery (38). Korrespondenzadresse Dr. med. Fabio Dennstädt Klinik für Radioonkologie Kantonsspital St. Gallen Rorschacher Strasse 95 9007 St. Gallen E-Mail: fabio.dennstaedt@kssg.ch Prof. Dr. Paul Martin Putora Klinik für Radioonkologie Kantonsspital St. Gallen Dr. Pawel Leskow Klinik für Thoraxchirurgie Kantonsspital St. Gallen Conflict of interest: None References: 1. Krebs in der Schweiz: Wichtige Zahlen. Krebsliga Schweiz https://www.krebs- liga.ch/ueber-krebs/zahlen-fakten/-dl-/fileadmin/downloads/sheets/zahlenkrebs-in-der-schweiz.pdf 2. Bericht des Bundesamts für Statistik über Lungenkrebs. https://www.bfs. admin.ch/bfs/de/home/statistiken/gesundheit/gesundheitszustand/krankheiten/krebs/spezifische.assetdetail.20744807.html 3. Ruano-Raviña Aet al.: Lung cancer symptoms at diagnosis: results of a nationwide registry study. ESMO Open. 2020;5(6):e001021. 4. Spiro SG et al.: Initial Evaluation of the Patient With Lung Cancer: Symptoms, Signs, Laboratory Tests, and Paraneoplastic Syndromes. Chest. 2007; 132(3):149S-160S. 5. Goldstraw P et al.: The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11(1):39-51. 6. Onkopedia Guideline for Non-Small Cell Lung Cancer. Deutsche Gesellschaft für Hämatologie und Medizinische Onkologie e.V. https://www.onkopedia. com/de/onkopedia/guidelines/lungenkarzinom-nicht-kleinzellig-nsclc/@@ guideline/html/index.html 7. Duma N et al.: Non–Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin Proc. 2019;94(8):1623-1640. 8. Travis WD et al.: The 2015 World Health Organization Classification of Lung Tumors. J Thorac Oncol. 2015;10(9):1243-1260. 9. Simon M et al.: Pulmonary nodules as incidental findings. Can Med Assoc J. 2018;190(6):E167-E167. 10. Leitlinien Prävention, Diagnostik, Therapie und Nachsorge des Lungenkarzinoms. Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V. https://www.awmf.org/leitlinien/detail/ll/020-007OL.html 11. Guideline Early Stage Non-Small Cell Lung Cancer. National Comprehensive Cancer Network. https://www.nccn.org/patients/guidelines/content/PDF/ lung-early-stage-patient.pdf 12. Roy P.: Preoperative pulmonary evaluation for lung resection. J Anaesthesiol Clin Pharmacol. 2018;34(3):296. 13. Migliore M et al.: Ground glass opacities management in the lung cancer screening era. Ann Transl Med. 2018;6(5):90-90. 14. Handa Y et al.: Transition of Treatment for Ground Glass Opacity–Dominant Non-Small Cell Lung Cancer. Front Oncol. 2021;11:655651. 15. Fang W.: Commentary: Is segmentectomy ready to be accepted as the standard of care? J Thorac Cardiovasc Surg. 2021;161(1):292-293. 16. Vansteenkiste J et al.: 2nd ESMO Consensus Conference on Lung Cancer: early-stage non-small-cell lung cancer consensus on diagnosis, treatment and follow-up. Ann Oncol. 2014;25(8):1462-1474. 17. Yang CFJ et al.: A National Analysis of Long-term Survival Following Thoracoscopic Versus Open Lobectomy for Stage I Non-small-cell Lung Cancer. Ann Surg. 2019;269(1):163-171. 18. Tong Y et al.: Characteristics of Postoperative Pain After VATS and Pain-Related Factors: The Experience in National Cancer Center of China. J Pain Res. 2020;Volume 13:1861-1867. 19. Watanabe S et al.: Lymph Node Dissection for Lung Cancer: Significance, Strategy, and Technique. J Thorac Oncol. 2009;4(5):652-657. 20. Tsutani Y et al.: Oncologic outcomes of segmentectomy compared with lobectomy for clinical stage IA lung adenocarcinoma: Propensity score–matched analysis in a multicenter study. J Thorac Cardiovasc Surg. 2013;146(2):358-364. 21. Raman V et al.: Surgical treatment for early stage non-small cell lung cancer. J Thorac Dis. 2018;10(S7):S898-S904. 22. Ziarnik E et al: Postlobectomy Early Complications. Thorac Surg Clin. 2015;25(3):355-364. 23. Frendl G et al.: 2014 AATS guidelines for the prevention and management of perioperative atrial fibrillation and flutter for thoracic surgical procedures. Executive summary. J Thorac Cardiovasc Surg. 2014;148(3):772-791. 24. Wen Z et al.: Comparison of outcomes following segmentectomy or lobectomy for patients with clinical N0 invasive lung adenocarcinoma of 2 cm or less in diameter. J Cancer Res Clin Oncol. 2020;146(6):1603-1613. 25. Benderli Cihan Y.: The Place and Importance of SBRT in Early Stage NSCLC. Turk Thorac J. 2021;22(5):424-425. 26. Timmerman R.: Stereotactic Body Radiation Therapy for Inoperable Early Stage Lung Cancer. JAMA. 2010;303(11):1070. 27. Haque W et al.: Stereotactic body radiation therapy versus conventionally fractionated radiation therapy for early stage non-small cell lung cancer. Radiother Oncol. 2018;129(2):264-269. 28. Brada M et al.: SABR in NSCLC – The beginning of the end or the end of the beginning? Radiother Oncol. 2015;114(2):135-137. 29. Guckenberger M et al.: ESTRO ACROP consensus guideline on implementation and practice of stereotactic body radiotherapy for peripherally located early stage non-small cell lung cancer. Radiother Oncol. 2017;124(1):11-17. 30. Kong FM et al.: High-dose radiation improved local tumor control and overall survival in patients with inoperable/unresectable non–small-cell lung cancer: Long-term results of a radiation dose escalation study. Int J Radiat Oncol. 2005;63(2):324-333. 31. Thompson M et al.: The evolving toxicity profile of SBRT for lung cancer. Transl Lung Cancer Res. 2018;8(1):48-57. 32. Grutters JPC et al.: Comparison of the effectiveness of radiotherapy with photons, protons and carbon-ions for non-small cell lung cancer: A meta-analysis. Radiother Oncol. 2010;95(1):32-40. 33. Randomized Study to Compare CyberKnife to Surgical Resection In Stage I Non-small Cell Lung Cancer (STARS). https://clinicaltrials.gov/ct2/show/ NCT00840749 34. Trial of Either Surgery or Stereotactic Radiotherapy for Early Stage (IA) Lung Cancer (ROSEL). https://clinicaltrials.gov/ct2/show/NCT00687986 35. Chang JY et al.: Stereotactic ablative radiotherapy versus lobectomy for operable stage I non-small-cell lung cancer: a pooled analysis of two randomised trials. Lancet Oncol. 2015;16(6):630-637. 36. Albano D et al.: 1-, 3-, and 5-year survival among early-stage lung cancer patients treated with lobectomy vs SBRT. Lung Cancer Targets Ther. 2018;9:65-71. 37. Detillon DDEMA et al.: Video-assisted thoracic lobectomy versus stereotactic body radiotherapy for stage I nonsmall cell lung cancer in elderly patients: a propensity matched comparative analysis. Eur Respir J. 2019;53(6):1801561. 38. Shinde A et al.: Stereotactic body radiation therapy (SBRT) for early-stage lung cancer in the elderly. Semin Oncol. 2018;45(4):210-219. 10 SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 5/2022