Transkript
Field experience report
First clinical experience with trastuzumab deruxtecan in Switzerland
An online survey among oncologists
URS BREITENSTEINA*, BASIL BÄTTIGBC, BARBARA BOLLIGERD, MICHELE CIRIOLOE, MATTHIAS EGGERF, URSULA HASLER-STRUBG, JENS HUOBERH, CATRINA UHLMANN NUSSBAUMI, MARCUS VETTERJ, KHALIL ZAMANK*
Background
Breast cancer is the most common type of cancer worldwide (1). In Switzerland, more than 6000 women are diagnosed every year (2). In 15–20 % of all breast cancers, the human epidermal growth factor receptor 2 (HER2) gene is amplified, overexpressed, or both (3). In these patients, the risk of metastases and recurrence is higher and outcomes have historically been poor, until HER2-targeted therapies including monoclonal antibodies, tyrosine kinase inhibitors (TKIs), and antibody-drug conjugates (ADCs) have revolutionized patients’ treatment and improved survival rates (3). As first-line regimen for patients with newly diagnosed metastatic HER2-positive breast cancer, current guidelines recommend dual HER2-blockade with the monoclonal antibodies trastuzumab and pertuzumab in combination with a taxane, based on the results of the CLEOPATRA trial (4). As an advancement of anti-HER2 antibodies, ADCs offer a combination of tumor-antigen specificity and the potent cytotoxicity of chemotherapeutic agents, allowing for increased activity at tumor sites. The ADC trastuzumab emtansine (T-DM1) combines HER2-targeting with the cytotoxic microtubule inhibitor maytansine. Until now, it was standard practice for second-line treatment based on a significant improvement of progression free survival (PFS) and overall survival (OS) compared with lapatinib/capecitabine in the pivotal phase III trial EMILIA (5). Beyond second line treatment, however, an universal consensus on best practice does not exist due to lack of randomized controlled trial data. Understanding resistance mechanisms remains a major challenge in defining optimal treatment sequences, especially with more effective agents becoming available. Currently, in later therapeutic lines, HER2blockade with trastuzumab beyond progression or TKIs are often maintained in combination with chemotherapy or endocrine therapy, with limited benefit in this advanced setting (6). In hormone receptorpositive (HR+) cases, endocrine treatment in combination with trastuzumab is an additional option.
Trastuzumab deruxtecan (T-DXd) is a next-generation ADC with different characteristics, including a higher antibody-to-drug ratio as compared to older ADCs. It combines HER2-targeting and the cytotoxic topoisomerase I inhibitor deruxtecan with a tumor-specific, cleavable linker (7). Deruxtecan is cell membrane permeable, allowing it to reach neighboring cancer cells, even if they do not express HER2 (bystander effect). In the multicenter open-label phase II trial DESTINY-Breast01 with 184 heavily pretreated patients with HER2positive metastatic breast cancer, who had progressed under T-DM1, T-DXd achieved unprecedented response rates (8). Based on the results of this trial, T-DXd was approved for the treatment of unresectable or metastatic HER2-positive breast cancer after at least two prior lines of HER2-targeted therapies in December 2019 in the United States and in January 2021 in Europe. At the time of the survey (November 2021), the drug was approved in Switzerland for the treatment of adult patients with unresectable locally advanced or metastatic HER2-positive breast cancer who have received at least two HER2-directed treatment regiments, including trastuzumab, and have had disease progression during or after therapy with T-DM1.+ Further clinical trials are investigating TDXd in earlier lines of therapy. The open-label, randomized phase III trial DESTINY-Breast03 (NCT03529110) evaluated T-DXd in a head-tohead comparison versus T-DM1 in 524 patients previously treated with trastuzumab and taxane in second or later therapy lines. In this trial, T-DXd showed a significant improvement in PFS: while the median PFS was not reached in the T-DXd group (95% CI: 18.5–not estimable), PFS in the T-DM1 group was 6.8 months (95% CI: 5.6–8.2) (9). OS data are currently not mature. At 12 months, the percentage of patients who were alive without disease progression was 75.8% (95% CI: 69.8–80.7) in patients who received T-DXd and 34.1% (95% CI: 27.7–40.5) in patients who received T-DM1.
a Brust-Zentrum Zürich, b Practice Onkologie Bellevue, Zürich, c Oncology Department, Spital Zollikerberg, Zürich, d Tumor- und Brustzentrum ZeTuP, St. Gallen, e Bürgerspital Solothurn, f Tumorzentrum ZeTuP, Rapperswil-Jona, g Kantonsspital Graubünden, Chur, h Kantonsspital St. Gallen, St. Gallen, i Kantonsspital Olten,
Olten, j Kantonsspital Baselland, Liestal, k Lausanne University Hospital CHUV, Lausanne,* Contributed equally to this study
34 SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 4/2022
Field experience report
Abstract
Summary
BACKGROUND: HER2 is a prime example of how discovering and targeting oncogenic drivers can revolutionize clinical practice and achieve unprecedented outcomes. A new generation of HER2-targeted agents is now tackling the inherent challenges of drug resistance and lack of treatment options in later therapeutic lines in HER2-positive and HER2-low breast cancer. One of these agents is the antibody-drug conjugate trastuzumab deruxtecan, which has been approved in Switzerland in November 2021.
OBJECTIVES: Selected patients in Switzerland had access to trastuzumab deruxtecan before its approval. The aim of this survey was to document the first clinical experiences and insights that treating oncologists obtained with trastuzumab deruxtecan therapy and management. These data could be informative for the future prescribers.
METHODS: An online survey with 25 questions was distributed to 17 breast oncologists across Switzerland, whose patients either had early access to trastuzumab deruxtecan by participating in a compassionate use program, a clinical trial with trastuzumab deruxtecan, or upon agreement of the patient’s health insurance. The survey was open for 17 days, from November 12th to November 29th, 2021.
RESULTS: 11 oncologists completed the survey (response rate: 64.7%), representing a total of 25 patients treated in private practices, regional hospitals, university hospitals, as well as certified breast cancer centers. Seventeen patients (68%) received trastuzumab deruxtecan in a compassionate use program. Four patients (16%) with HER2-low expressing metastatic breast cancer (IHC 1+ or 2+, ISH negative) were enrolled in the phase III trial DESTINY-Breast04. Four patients (16%) obtained access to trastuzumab deruxtecan via request to their health insurances. T-DXd was most commonly (40%) administered as third-line treatment. Prior to trastuzumab deruxtecan, all patients with HER-2-positive disease (IHC 3+ or ISH-confirmed) had been exposed to a HER2-targeting monoclonal antibody, i.e., trastuzumab, pertuzumab or both. 80% of them were exposed to trastuzumab emtansine and 80% had been exposed to a tyrosine kinase inhibitor. Adverse events specified most were hematotoxicity (32%), alopecia (28%), nausea (24%), and fatigue (20%). Treatment-emergent interstitial lung disease occurred in 8% of the patients and required treatment discontinuation. 44% discontinued treatment, mainly due to progressive disease and interstitial lung disease.
CONCLUSION: The first patients who have been treated with trastuzumab Deruxtecan in Switzerland and are represented in this survey differed from the participants of the pivotal clinical trials DESTINY-Breast01 and DESTINY-Breast03 with regards to various baseline characteristics including age, performance status, comorbidities, and expression levels of HER2 and hormone receptors. Yet, the treatment experience with trastuzumab deruxtecan was largely consistent with the findings obtained in the pivotal clinical trials DESTINY-Breast01 and DESTINY-Breast03 with regards to side effects and therapy management. The treatment strategy for HER2-positive metastatic breast cancer specified by the participating oncologists reflects that of international guidelines, i.e., initial dual HER2-blockade combined with chemotherapy in the first line of treatment, followed by trastuzumab emtansine in the second line and a tyrosine kinase inhibitor, or, if accessible, trastuzumab deruxtecan in the third line of treatment.
Selected patients in Switzerland had access to T-DXd before its approval, typically through clinical trials and compassionate use programs. In this report, we share the first clinical experiences and insights that we and other treating oncologists have acquired with T-DXd, as well as the challenges that were encountered with regards to T-DXd management.
Methods
Survey design and study sample To obtain numerically evaluable data, a survey with 25 questions was distributed via e-mail to 17 breast oncologists across Switzerland, whose patients either had early access to T-DXd by participating in a compassionate use program, a clinical trial with TDXd, or upon agreement of the patient’s health insurance.
Questionnaire The questionnaire was developed by the medical communication agency IACULIS GmbH in collaboration with the authors UB and KZ. The survey consisted of 25 questions in English language and required 15–20 minutes to complete. The survey comprised both multiple choice and free text questions (see supplementary Appendix). The setup and analysis of the survey provided for physician and patient anonymity.
Analysis Results are presented either as total values or as percentage of total patients or a subset of patients, as indicated. The survey was neither designed nor intended to enable statistical evaluations on T-DXd’s efficacy and safety. Hence, statistical means of analysis were not applied.
SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 4/2022
35
Field experience report
Results
Response rate and background information on treating oncologists By the data cut-off on November 29th, 2021, 11 oncologists had completed the questionnaire (response rate 64.7%), representing a total of 25 patients. Nine of the responding oncologists administered T-DXd in the setting of a compassionate use program (17 patients, 68%). One reported that their patients (n = 4, 16%) were enrolled in the phase III trial DESTINY-Breast04 (NCT03734029), which examines the efficacy of T-DXd in HER2-low expressing metastatic breast cancer (HER2 IHC 1+
Table 1 BASELINE CHARACTERISTICS
patients represented DESTINY-
in this survey
Breast01
(n = 25)
(n = 184) (8)
DESTINY-Breast03, T-DXd arm (n = 261) (9)
Median age, years female
median spana: 60–70
100%
Race
White 100%
Asian 0.0%
Other or missing data 0.0%
HR+ disease
68.0%
HER2 expression
IHC 3+ ≥40%*
IHC 1+ ≥28%*
ECOG performance status
0 54.2%
1 33.3%
2 12.5%
Comorbidities
Brain metastases
treated, asymptomatic 32.0%
active 4.0%
visceral disease
92.0%
cardiac dysfunction
0.0%
liver dysfunction
16.0%
renal dysfunction
4.0%
55
100%
54.9% 38.0% 7.1% 53.0%
83.7% 15%**
55.4% 44.0% 0.2%±
13.0% 0.0%± 91.8% n/s n/s n/s
54.3
99.6%
n/s n/s n/s 50.2%
89.7% 0.4%
59.0% 40.6% 0%±
23.8% 0.0%± 70.5% n/s n/s n/s
Baseline characteristics of patients represented in this survey (answers from 11 oncologists, representing 25 patients) and participants of the DESTINY-Breast01 trial and the T-DXd-arm of the DESTINY-Breast03 trial. * aage options in this survey: <20, 20–30, 30–40, 40–50, 50–60, 70–80, >80; IHC information on 8 patients with ISH+ disease is missing. Therefore, percentages might be higher. **patients with IHC 1+ or IHC2+ and ISH+ disease. ECOG: Eastern Cooperative Oncology Group scale; HR+: hormone receptor-positive; IHC: immunohistochemistry; ISH: in situ hybridization; n/s: not specified.
or 2+). One oncologist obtained access to T-DXd via request to the patients’ (n = 4, 16%) health insurances. Responding oncologists were practicing in private practices (30.8%), certified breast cancer centers (46.2%), university hospitals (23.1%), and regional hospitals (28.1%) across Switzerland (multiple answers were possible).
Baseline characteristics of patients represented in this survey All baseline characteristic and comorbidities assessed in this survey are summarized in Table 1. The patients treated in Switzerland were at least 30 years of age, with the majority being 50–60 (32%) and 60– 70 (32%) years old. 32% of the patients (n=8) had an amplification of HER2 demonstrated by in situ hybridization (ISH). In those patients, information on the immunohistochemistry (IHC) status was not covered by the survey. Among the 17 patients whose HER2status was specified via IHC scores, 10 had a score of 3+ (40% of all patients, 58.8% of IHC-assessed patients), none had a score of 2+, and 7 patients had a score of 1+ (28% of all patients, 41,2% of IHC-assessed patients).
Comorbidities 32% of the patients represented in this survey have a history of brain metastases and one patient (4%) had active brain metastases during T-DXd therapy (Table 1). None of the patients suffered from significant cardiac dysfunction. Liver dysfunction affected 16% and renal dysfunction affected 4% of the patients. Other comorbidities specified via free text answers in this survey included diabetes, hypertension, psychiatric disease and pulmonary embolism.
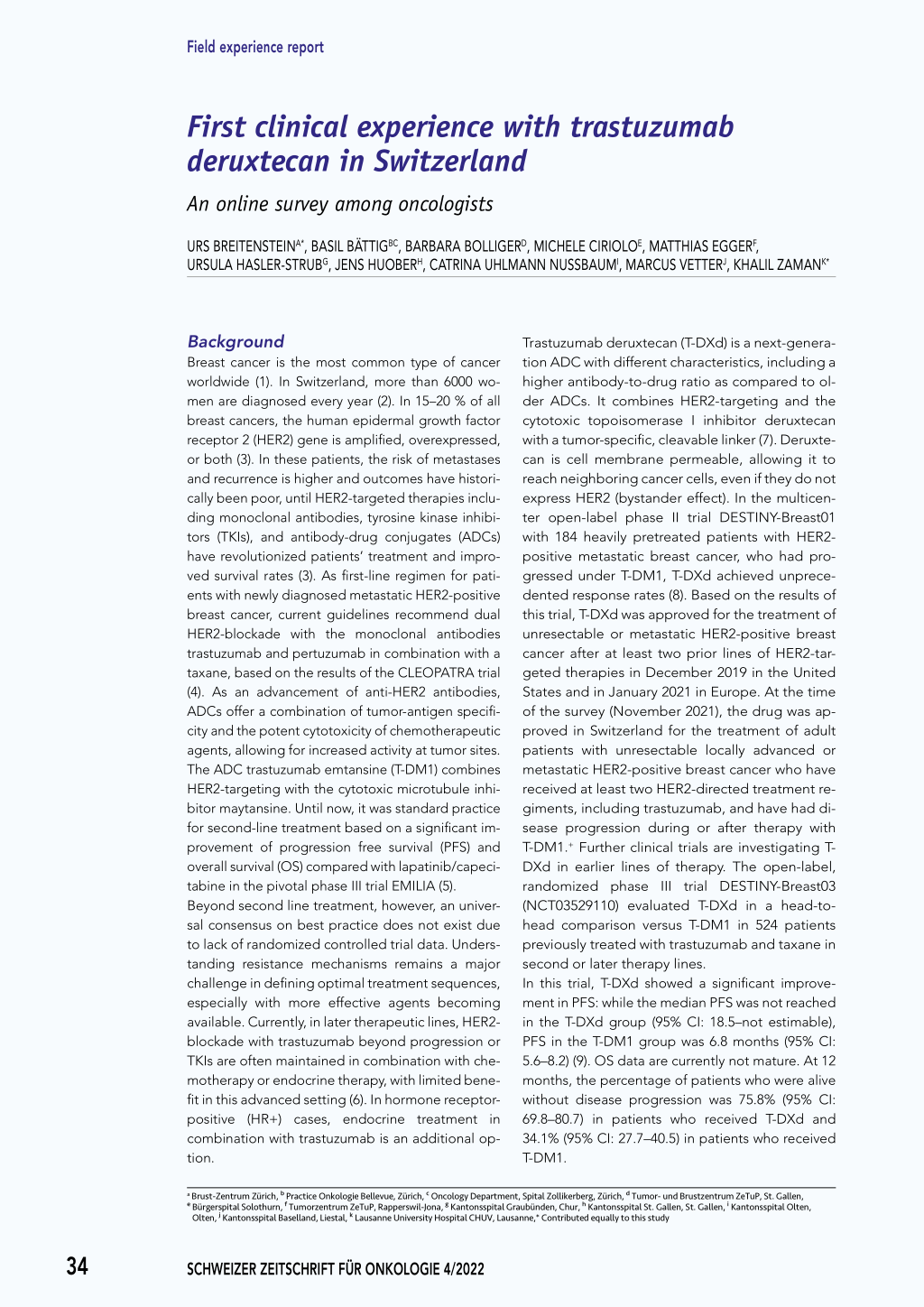
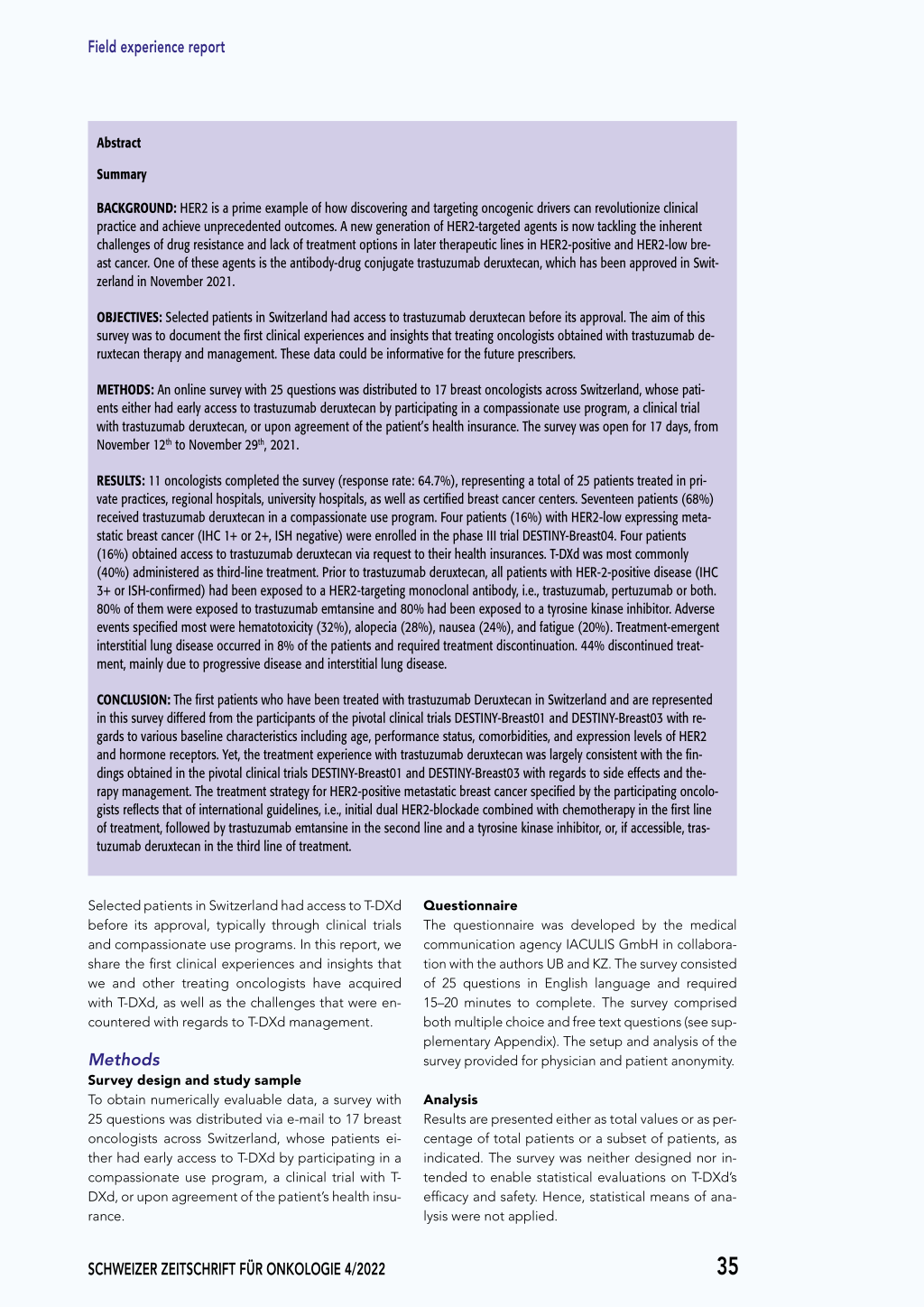
T-DXd was mainly used in the third treatment line, after trastuzumab, pertuzumab and T-DM1 The patients represented in this survey received T-DXd mainly in the third treatment line (40.0%), followed by the fourth (24.0%) (Figure 1). Specific information on first-line treatment is available for 16 patients. Three of those had HER2-low expressing disease (IHC 1+) and 13 had HER2-positive disease as confirmed by IHC 3+ or ISH. In 61.5% of the 13 patients with HER2-positive disease, firstline treatment was dual HER2-blockade with trastuzumab and pertuzumab, in 23.1% trastuzumab monotherapy, and 15.4% received pertuzumab monotherapy (Figure 2A). For 9 HER2-positive patients, second-line treatment information is available. Among those, 77.8% received T-DM1 (Figure 2B). The remaining patients received either second-line endocrine therapy (11.1%) or pertuzumab (11.1%).
36 SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 4/2022
Field experience report
Third-line treatment has been specified for 7 pati-
ents with HER2-positive diseaseF.igTuhres1e: patients
mainly received HER2-directed TKIs (62.5%), T-DM1 (14.3%) or a combination of both (14.3%) (Figure 2C). For 5 HER2-positive metastatic breast cancer patients, the complete regimen of previous treatment lines prior to T-DXd is available: All these patients received trastuzumab, pertuzumab or both (Figure 2D). 80% were exposed to T-DM1, and 80% were exposed to an anti-HER2 TKI prior to T-DXd therapy. Patients with HER2-low expressing metastatic breast cancer (IHC 1+) received chemotherapy without HER2-targeting as first-line therapy (n = 2), followed by endocrine therapy (n = 1) prior to T-DXd therapy. Another patient with IHC 1+ disease was treated with trastuzumab as first-line therapy, followed by T-DM1 and a TKI, before she received T-DXd. For the other 4 patients with HER2-low disease in this survey, no information on previous therapies was specified.
A
30%
HER2-positive mBC (IHC 3+ or ISH-confirmed) In which metastatic line did you administer
trastuzumab deruxtecan?
% of patients with HER2+ mBC
25%
20%
15%
10%
5%
0% 1 2 3 4 5 6 7 8 9 10
treatment line
B
100%
HER2-low mBC (IHC 1+ ) In which metastatic line did you administer
trastuzumab deruxtecan?
80%
60%
40%
% of patients with HER2-low mBC
20%
Most common adverse events were
hematotoxicity, alopecia, nausea, and fatigue Treatment-emergent adverse events (TEAEs) of
0% 1 2 3 4 5 6 7 8 9 10
treatment line
any grade as specified by free text answers were
hematotoxicity (not further specified), alopecia, nausea, fatigue, asthenia, weight loss, and diarrhea (Table 2). Five patients (20%) did not experience any side effects during T-DXd therapy. T-DXd therapy is associated with a 0.5–15% risk of interstitial
Figure 1: T-DXd administration by treatment line in patients with HER2-positive and HER2-low expressing disease, respectively. Graphs show percentage of (A) 18 patients with HER2-positive disease (IHC 3+ or ISH-confirmed) and (B) 7 patients with HER2-low disease (IHC 1+). ISH: in situ hybridization; mBC: metastatic breast cancer.
lung disease (10), which also occurred in 8% of the
patients represented in this survey and required Figure 2: Previous systemic therapies in HER2+ patients (IHC 3+ or ISH+)
treatment discontinuation. TEAEs required dose reductions in 20% of patients and treatment discontinuation in 12%.
FigureA2: Previous systemic therapies
first line
A(% of 13 patients with HER2+ mBC)
15.4% first line
in
HER2+
patienBts
(IHC
3+ or ISH+)
second line
(% of 9 patients with HER2+ mBC)
B 11.s1e%cond1l1in.1e%
Most patients (88%) started T-DXd treatment with
(% of 13 patients with HER2+ mBC)
15.4%
du al blockade
(% of 9 patients with HER2+ mBC)
11.1% 11.1%
endocrine therapy
the recommended starting dose of 5.4 mg/kg ad- 23.1%
trastuzumab
T-DM1
ministered in the pivotal T-DXd trials (8, 9). For three patients (12%), lower starting doses were adminis-
23.1%
61.5% 61.5%
dpuearltublzoucmkaadbe trastuzumab
pertu zumab
77.8%
epnedrtouczruinmeatbherapy T-DM1
pertu zumab
tered, due to bone marrow toxicity of a prior therapy, impaired liver function, and limited availability of the drug, respectively, as specified by free text answers.
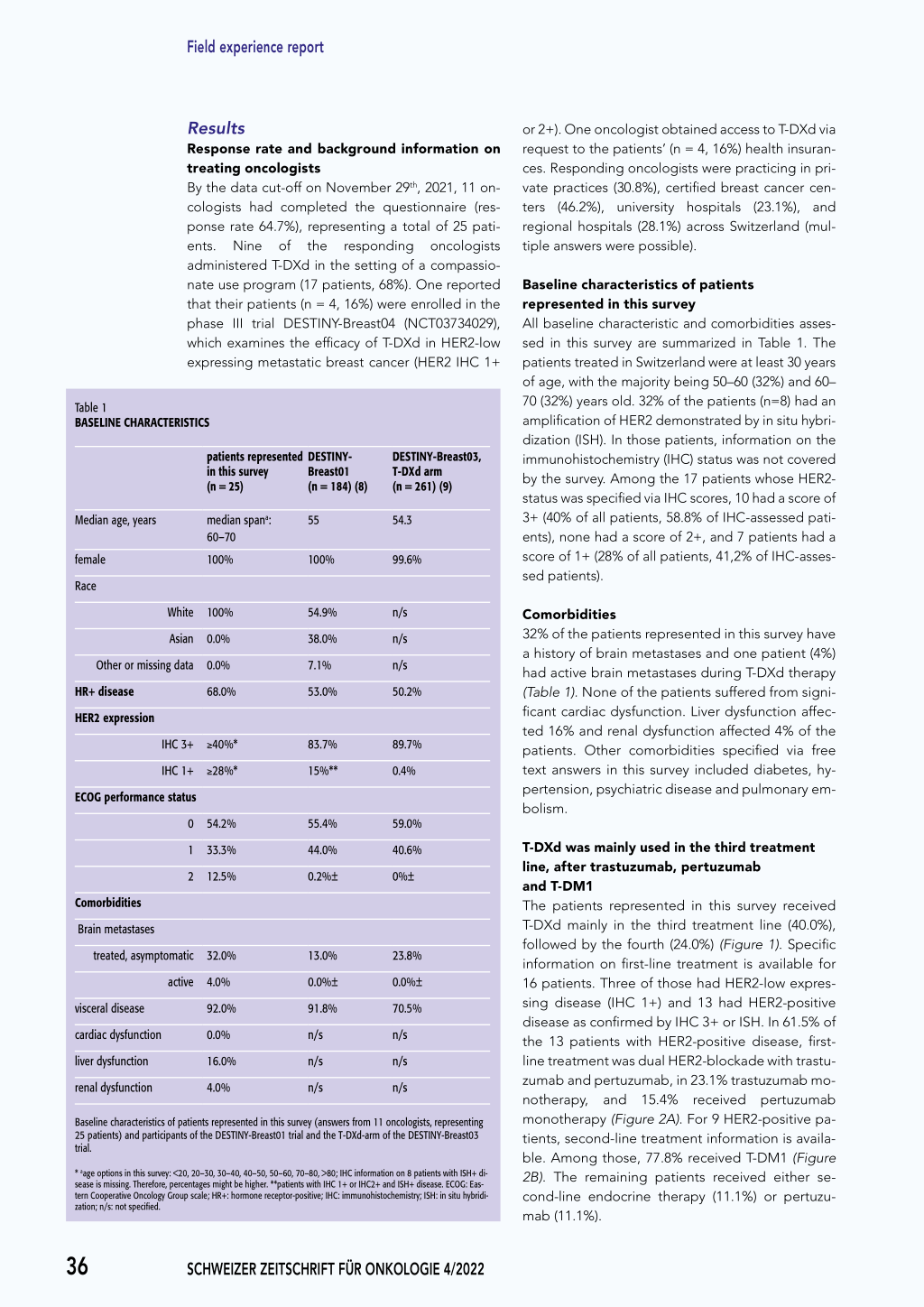
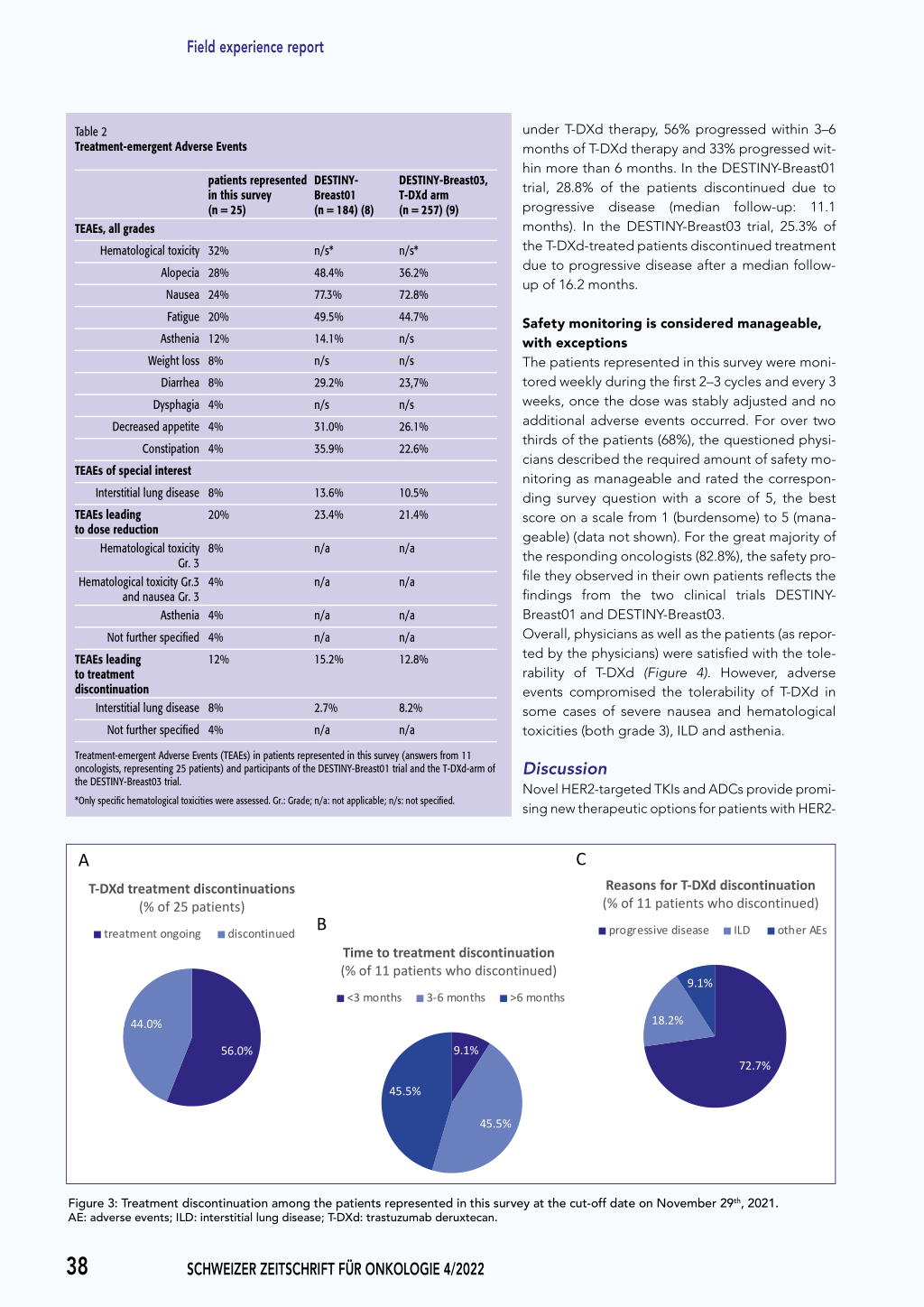
Treatment discontinuation rate and disease progression Upon data cut-off on November 29, 2021, responding oncologists indicated that 44% of the patients (n = 11) had discontinued T-DXd treatment (Figure 3A). The majority of the respondents specified the
77.8%
C D Exposure to previous agents before T-DXd
third line
(5 patients with HER2+ mBC)
C (% of 7 patients with HER2+ mBC)
D 100.0% Exposure to previous agents before T-DXd
14.3%third line
80.0%
(5 patients with HER2+ mBC)
(% of 7 patients with HER2+ mBC)
14.3%
TKI
10600..00%%
14.3%
T-DM1 + TKI
8400..00%%
patients (p%a)tients (%)
62.5%
TTK-IDM1
6200..00%%
14.3%
T-DM1 + TKI
400..00%%
62.5%
T-DM1
20.0% 0.0%
pertuzumab, trastuzumab or du al blockade pertuzumab, trastuzumab or du al blockade
T-DM1 T-DM1
anti-HER2 TKI anti-HER2 TKI
time to treatment discontinuation as 3–6 months or more than 6 months (both 45.5% of patients who discontinued T-DXd). For 36% of all patients (n = 9), disease progression under T-DXd therapy was reported. All of them discontinued treatment. Of the 9 patients who suffered from disease progression
Figure 2: Previous systemic therapies in HER2-positive metastatic breast cancer patients represented in this survey (IHC 3+ or ISH-confirmed). A-C: Graphs show percentage of patients for whom first to third line regimens were specified by the responding oncologists. D: Complete regimens for all treatment lines prior to T-DXd were available for 5 patients. HER2+: HER2-positive; mBC: metastatic breast cancer; T-DM1: trastuzumab
emtansine; T-DXd: trastuzumab deruxtecan; TKI: tyrosine kinase inhibitor.
SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 4/2022
37
Field experience report
Table 2 Treatment-emergent Adverse Events
TEAEs, all grades
patients represented DESTINY-
in this survey
Breast01
(n = 25)
(n = 184) (8)
Hematological toxicity 32%
n/s*
Alopecia 28%
48.4%
Nausea 24%
77.3%
Fatigue 20%
49.5%
Asthenia 12%
14.1%
Weight loss 8%
n/s
Diarrhea 8%
29.2%
Dysphagia 4%
n/s
Decreased appetite 4%
31.0%
Constipation 4%
35.9%
TEAEs of special interest
Interstitial lung disease 8%
13.6%
TEAEs leading to dose reduction
20%
Hematological toxicity 8% Gr. 3
Hematological toxicity Gr.3 4% and nausea Gr. 3
Asthenia 4%
23.4% n/a n/a n/a
Not further specified 4%
n/a
TEAEs leading to treatment discontinuation
12%
Interstitial lung disease 8%
15.2% 2.7%
Not further specified 4%
n/a
DESTINY-Breast03, T-DXd arm (n = 257) (9)
n/s* 36.2% 72.8% 44.7% n/s n/s 23,7% n/s 26.1% 22.6%
10.5% 21.4%
n/a
n/a
n/a n/a 12.8%
8.2% n/a
under T-DXd therapy, 56% progressed within 3–6 months of T-DXd therapy and 33% progressed within more than 6 months. In the DESTINY-Breast01 trial, 28.8% of the patients discontinued due to progressive disease (median follow-up: 11.1 months). In the DESTINY-Breast03 trial, 25.3% of the T-DXd-treated patients discontinued treatment due to progressive disease after a median followup of 16.2 months.
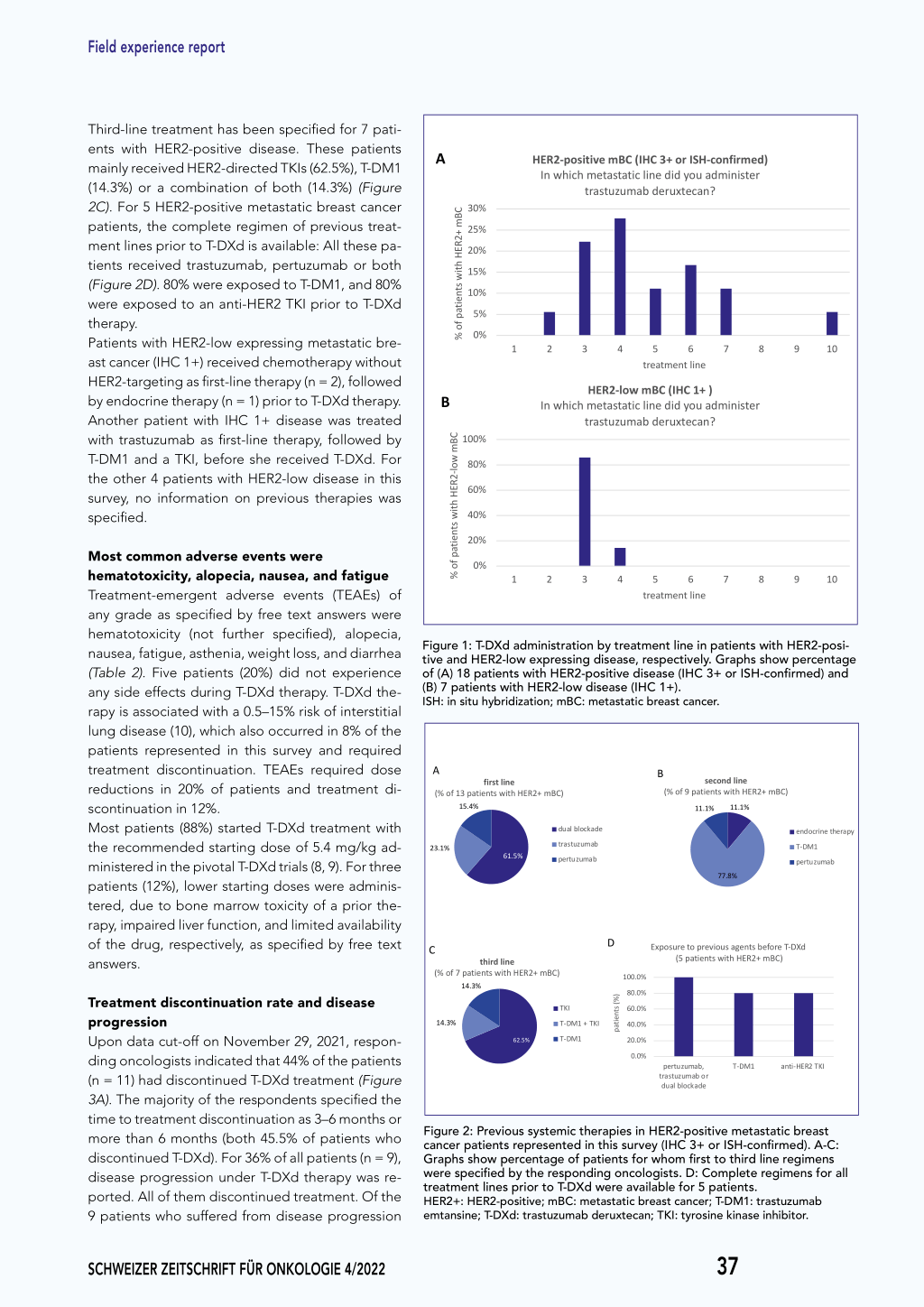
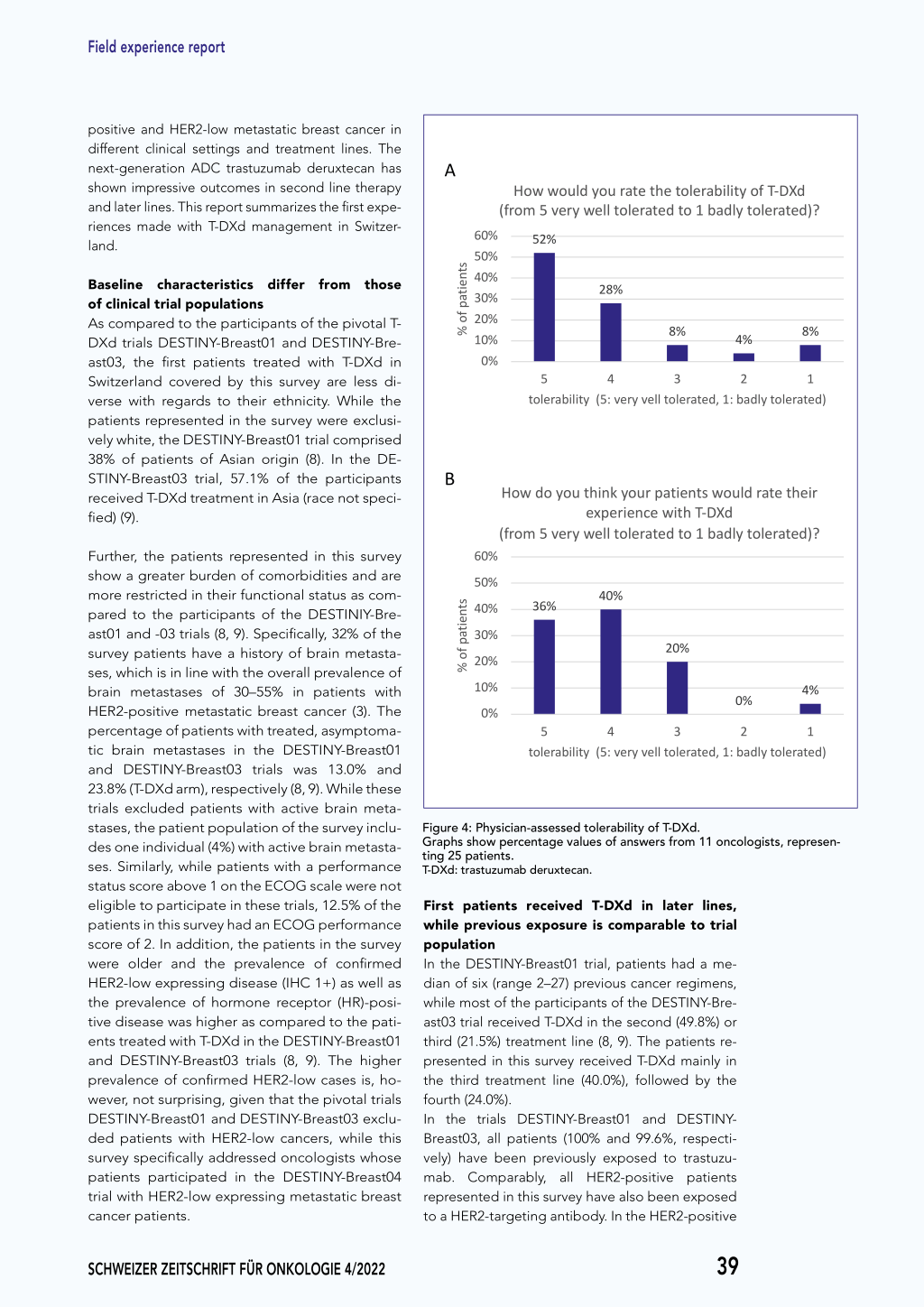
Safety monitoring is considered manageable, with exceptions The patients represented in this survey were monitored weekly during the first 2–3 cycles and every 3 weeks, once the dose was stably adjusted and no additional adverse events occurred. For over two thirds of the patients (68%), the questioned physicians described the required amount of safety monitoring as manageable and rated the corresponding survey question with a score of 5, the best score on a scale from 1 (burdensome) to 5 (manageable) (data not shown). For the great majority of the responding oncologists (82.8%), the safety profile they observed in their own patients reflects the findings from the two clinical trials DESTINYBreast01 and DESTINY-Breast03. Overall, physicians as well as the patients (as reported by the physicians) were satisfied with the tolerability of T-DXd (Figure 4). However, adverse events compromised the tolerability of T-DXd in some cases of severe nausea and hematological toxicities (both grade 3), ILD and asthenia.
Treatment-emergent Adverse Events (TEAEs) in patients represented in this survey (answers from 11
3 Figure 3oncologists, representing 25 patients) and participants of the DESTINY-Breast01 trial and the T-DXd-arm of the DESTINY-Breast03 trial.
Discussion
Novel HER2-targeted TKIs and ADCs provide promi-
*Only specific hematological toxicities were assessed. Gr.: Grade; n/a: not applicable; n/s: not specified.
sing new therapeutic options for patients with HER2-
Figure 3
A BB
CC
DtrXedattmAre(e%anttomofneg2no5tinTpdg-aDitstrXcieedoanntdttmtrissie(e)nc%anouttnaomottifnniego2uno5netidnspdgaistcieonndttissi)ncounattinioune(dTs%
T-DXd treatment discontinuations
Time to treatment discontinuation
Reasons for T-DXd discontinuation
(% of 25 patients)
treatment ongoing discontinued
(% of 11 patients who discontinued)
<3 months9.1% 3-6 months 9.1% >6 months
(% of 11 patients who discontinued)
progr9e.1ss%ive disease
9.1% ILD other AEs
44.0%
44.0% 56.0%
44.0%
56.0%
45.5%
45.5% 9.1%
45.5%
45.5%
45.5%
18.2%
18.2%
9.1% 72.7% 18.2%
72.7%
56.0%
45.5%
72.7%
Figure 3: Treatment discontinuation among the patients represented in this survey at the cut-off date on November 29th, 2021. AE: adverse events; ILD: interstitial lung disease; T-DXd: trastuzumab deruxtecan.
38 SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 4/2022
Field experience report
positive and HER2-low metastatic breast cancer in
different clinical settings and treatment lines. The
nexFt-iggeunreerat4FioinguArDeC4trastuzumab deruxtecan has A
shown impressive outcomes in second line therapy
andFliagteurrliene4Fs.iTghuisrerep4ort summarizes the first expe-
riences made with T-DXd management in Switzer-
A
land.
Baseline characteristics differ from those of clinical trial populations As compared to the participants of the pivotal TDXd trials DESTINY-Breast01 and DESTINY-Breast03, the first patients treated with T-DXd in Switzerland covered by this survey are less diverse with regards to their ethnicity. While the patients represented in the survey were exclusively white, the DESTINY-Breast01 trial comprised
B38% of patients of Asian origin (8). In the DE-
STINY-Breast03 trial, 57.1% of the participants
Breceived T-DXd treatment in Asia (race not speci-
fied) (9).
Further, the patients represented in this survey show a greater burden of comorbidities and are more restricted in their functional status as compared to the participants of the DESTINIY-Breast01 and -03 trials (8, 9). Specifically, 32% of the survey patients have a history of brain metastases, which is in line with the overall prevalence of brain metastases of 30–55% in patients with HER2-positive metastatic breast cancer (3). The percentage of patients with treated, asymptoma-
A
How Hwoowulwdoyuolud yraotuertahtee tthoeletroalebrilaibtyiliotyf To-fDTX-DdXd
A (from(f5rovmer5y vweeryllwtoellel rtaotleerdatteod1toba1dblaydtloylteorlaetreadte)?d)?
% of pati%eonftspatients % of pati%enoftspatients
60% 50%
(fr56Ho00%%mow(5f25rH%owvmoeow5ru25yl%wdvweoyeruoyllludwtyoreaolletluertoartatlheteeerdatttthoeoedle1ttrooableba1ridlabilbtayyidltioltoyyflteToor-flaDeTtrX-eaDddtXe)d?d)?
460% 350% 240% 130%
460% 350%52%
52%
240%
130%
20%
28% 28% 28% 28%
8% 8%
4% 4%
8% 8%
20% 10%
10% 0% 5
5 tolerabilit4y
4 (5: very
v8e3%ll to83l%erated,421%:
42% badly
tole8r1%a8t1e%d)
0% tolerabi5lity (5: very4vell tolera3ted, 1: badl2y tolerated1)
B HowtoHdl5eoorwaytboodiluleoitrytayhbo(ii5ulnit:4kytevheyx(i5rpony:ekuvvrreyeierolpylnuatvcorte3elilpeelwartnaotittliteeeshrdnawT,tte-s1oDd:wu,Xbl21oda:udbrllyaaddttreloyaltetteohraleetthr1eiaredtei)rd)
B
(Hfroowmd5ovyeeoxrupy ewthreiienllnktcoyeloeuwrarittpehadtTit-eoDnX1tsdbwaodulyldtorlaetreatehde)ir? (Hfr6oo0w%md5ovyeoruy wtheinllketoyxploeeurrarietpenadcteiteown1ittshbwTa-odDulXyldtorlaetreatehde)ir?
% of pati%eonftspatients % of pati%enoftspatients
60% 50%(from 5 veexrpyewreiellntcoelewraittehdTt-oDX1dbadly tolerated)?
50%(fr46o00%%m 5 ve3r6y%well to4le0%rated to 1 badly tolerated)?
60% 40% 50% 30% 40% 20% 30% 10% 20%
0% 10%
0%
3500%%36% 2400%% 1300%%36% 200%% 10%
0%
40% 36% 40%
40%
54 tolerability (5: very
20%
20% 20%
20% 3
0%
vell tolerated, 1:
0% 2 0b%adly
4%
4%41% tolerated)
5 5 44 toleratboilleitryab(i5lit:yve(5ry: vveerlyl
tvoe3llel rtao3tleerda,te1d: ,0b21%a:dbl2yadtloyletorale4tr1e%adt1e) d)
54321
tic brain metastases in the DESTINY-Breast01 and DESTINY-Breast03 trials was 13.0% and
tolerability (5: very vell tolerated, 1: badly tolerated)
23.8% (T-DXd arm), respectively (8, 9). While these
trials excluded patients with active brain meta-
stases, the patient population of the survey includes one individual (4%) with active brain metastases. Similarly, while patients with a performance status score above 1 on the ECOG scale were not
Figure 4: Physician-assessed tolerability of T-DXd. Graphs show percentage values of answers from 11 oncologists, representing 25 patients. T-DXd: trastuzumab deruxtecan.
eligible to participate in these trials, 12.5% of the patients in this survey had an ECOG performance score of 2. In addition, the patients in the survey were older and the prevalence of confirmed
First patients received T-DXd in later lines,
while previous exposure is comparable to trial
population In the DESTINY-Breast01 trial, patients had a me-
HER2-low expressing disease (IHC 1+) as well as dian of six (range 2–27) previous cancer regimens,
the prevalence of hormone receptor (HR)-posi- while most of the participants of the DESTINY-Bre-
tive disease was higher as compared to the pati- ast03 trial received T-DXd in the second (49.8%) or
ents treated with T-DXd in the DESTINY-Breast01 third (21.5%) treatment line (8, 9). The patients re-
and DESTINY-Breast03 trials (8, 9). The higher presented in this survey received T-DXd mainly in
prevalence of confirmed HER2-low cases is, ho- the third treatment line (40.0%), followed by the
wever, not surprising, given that the pivotal trials fourth (24.0%).
DESTINY-Breast01 and DESTINY-Breast03 exclu- In the trials DESTINY-Breast01 and DESTINY-
ded patients with HER2-low cancers, while this Breast03, all patients (100% and 99.6%, respecti-
survey specifically addressed oncologists whose vely) have been previously exposed to trastuzu-
patients participated in the DESTINY-Breast04 mab. Comparably, all HER2-positive patients
trial with HER2-low expressing metastatic breast represented in this survey have also been exposed
cancer patients.
to a HER2-targeting antibody. In the HER2-positive
SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 4/2022
39
Field experience report
population of this survey, the most common second-line treatment was T-DM1, followed by a HER2-targeting TKIs in the third line. Hence, the HER2-targeted approaches pursued by the participating physicians in Switzerland conforms with international guidelines. These recommend initial dual HER2-blockade combined with chemotherapy in the first line, followed by T-DM1 in the second line and a TKI, or, if accessible, T-DXd in the third line of treatment (4). These sequences can be modified for the patients having received some of these drugs in the adjuvant setting.
Distribution of adverse events is similar, although with lower overall prevalence Overall, the types of adverse events as well as the frequency of dose reductions specified in this survey are consistent with those observed in the DESTINYBreast01 trial and the T-DXd arm of the DESTINYBreast03 trial (8, 9). Specifically, hematotoxicity, nausea, fatigue, and alopecia were specified most in free text answers in this survey and were also the most abundant adverse events in the trials DESTINYBreast01 and -03 (8, 9). Of note, hematological adverse events reported in these trials were specified and categorized into lymphopenia, neutropenia, and thrombocytopenia, while the responses of this survey were not specified beyond the term «hematotoxicity».
Interstitial lung disease is a notable risk ILD is a critical risk for patients treated with T-DXd, requiring active surveillance and management. In the DESTINY-Breast01 and DESTINY-Breast03 trials, patients with a history of noninfectious ILD or pneumonitis requiring the use of glucocorticoids, or a current or suspected ILD or pneumonitis were excluded. 13.6% of the participants of the DESTINY-Breast01 trial developed ILD, which led to death in 16% of these patients (2.2% of the total patient population) (8). In the DESTINY-Breast03 trial, 10.5% of the patients who received T-DXd developed a drug-related ILD, with no ILD-related deaths reported (cutoff date: May 21, 2021) (9). In the patient population represented in this survey, 2 patients (8%) developed ILD, requiring for treatment discontinuation. Early diagnosis and intervention are key for optimal ILD management. Patients must be counseled and
educated to monitor and report respiratory symptoms such as cough, dyspnea, or even fever promptly.
Conclusion
Although patients represented in this survey differed from the participants in T-DXd clinical trials with regards to various baseline criteria, the first experiences oncologists obtained with T-DXd therapy in Switzerland are in accordance with the reports from the two pivotal T-DXd trials DESTINY-Breast01 and DESTINY-Breast03. While nausea, hematotoxicity, and ILD need to be monitored carefully and handled diligently, T-DXd was generally rated well tolerated. The overall safety profile was considered manageable by the respondents of this survey.
Acknowledgement: We thank all oncologists who participated in this survey.
Corresponding author Dr. Khalil Zaman Medical director Breast Center University Hospital CHUV, Lausanne khalil.zaman@chuv.ch
Funding sources and conflicts of interest: Daiichi Sankyo (Schweiz) AG and AstraZeneca AG have initiated and financially supported the survey and a subsequent meeting in which the outcome of the survey was discussed. Medical writing resources were also provided by Daiichi Sankyo (Schweiz) AG and AstraZeneca AG. The Sponsors had no influence on the content of the publication.
+Since June 2022, trastuzumab deruxtecan is approved in Switzerland for Monotherapy treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received at least one HER2-directed treatment regimen, including trastuzumab and a taxane, and have had disease progressive either at the metastatic stage or within 6 months of the end of adjuvant or neoadjuvant therapy.
Literatur 1. International Agency for Research on Cancer (IARC). https://gco.iarc.fr/today/
data/factsheets/cancers/20-Breast-fact-sheet.pdf. 2. Bundesamt für Statistik 2021. https://www.bfs.admin.ch/bfs/de/home/statisti-
ken/gesundheit/gesundheitszustand/krankheiten/krebs/spezifische.html. 3. Exman P et al.: HER2-positive metastatic breast cancer: A comprehensive re-
view. Clin. Adv. Hematol. Oncol 2021; 19: 40-50. 4. Cardoso F et al.: 5th ESO-ESMO international consensus guidelines for advan-
ced breast cancer (ABC 5). Annals of Oncology 2020; 31(12): 1623-1649. 5. Verma S et al.: Trastuzumab emtansine for HER2-positive advanced breast can-
cer. New England journal of medicine 2012; 367(19): 1783-1791. 6. Linehan AS et al.: Profile of Trastuzumab deruxtecan in the management of
patients with HER2-positive unresectable or metastatic breast cancer: an evidence-based review. Breast Cancer: Targets and Therapy 2021; 13: 151. 7. Perez J et al.: Trastuzumab deruxtecan in HER2-positive metastatic breast cancer and beyond. Expert Opinion on Biological Therapy 2021; 21(7): 811-824. 8. Modi S et al.: Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. New England Journal of Medicine 2020; 382(7): 610-621. 9. Cortés J et al.: Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer. New England Journal of Medicine 2022; 386(12): 1143-1154. 10. Tarantino P et al.: Interstitial lung disease induced by anti-ERBB2 antibodydrug conjugates: a review. JAMA oncology 2021; 7(12): 1873-1881.
40 SCHWEIZER ZEITSCHRIFT FÜR ONKOLOGIE 4/2022