

Transkript
FORTBILDUNG
Validity of the clinical examination in the diagnosis of Functional Neurological Symptoms (Conversion Disorder)
Deepa Pothalil Selma Aybek
von Deepa Pothalil1 und Selma Aybek2
Abstract:
D er Begriff der Hysterie existiert noch immer, auch wenn dieser durch weniger stigmatisierende Begriffe wie psychogene Störung, dissoziative Störung oder Konversionsstörung ersetzt wurde. In Zukunft wird dieser Begriff bald unter dem einheitlichen Begriff eines funktionellen neurologischen Symptoms zusammengefasst werden. Die Diagnostik ist äusserst schwierig, das unterstreicht die Bedeutung von positiven motorischen und sensorischen Zeichen. Durch die Ergebnisse der Neurobildgebung bahnt sich zudem in den letzten Jahren ein Paradigmenwechsel von einem primär psychologischen oder psychiatrischen zu einem neurologischen Krankheitsbild an. Das sorgt aus Sicht des Patienten für Sicherheit, der sich damit ernst genommen fühlt und nicht als Simulant wahrgenommen wird. Auf der ärztlichen Seiten führt die Validation anhand der positiven Symptome ebenfalls für mehr Sicherheit und nimmt die mögliche Angst vor einer Fehldiagnose. Eine wirksame Behandlung fehlt bislang. Der multidisziplinäre Ansatz mit einer Zusammenarbeit von Psychiatern als auch Neurologen scheint die Prognose des Patienten allerdings zu verbessern.
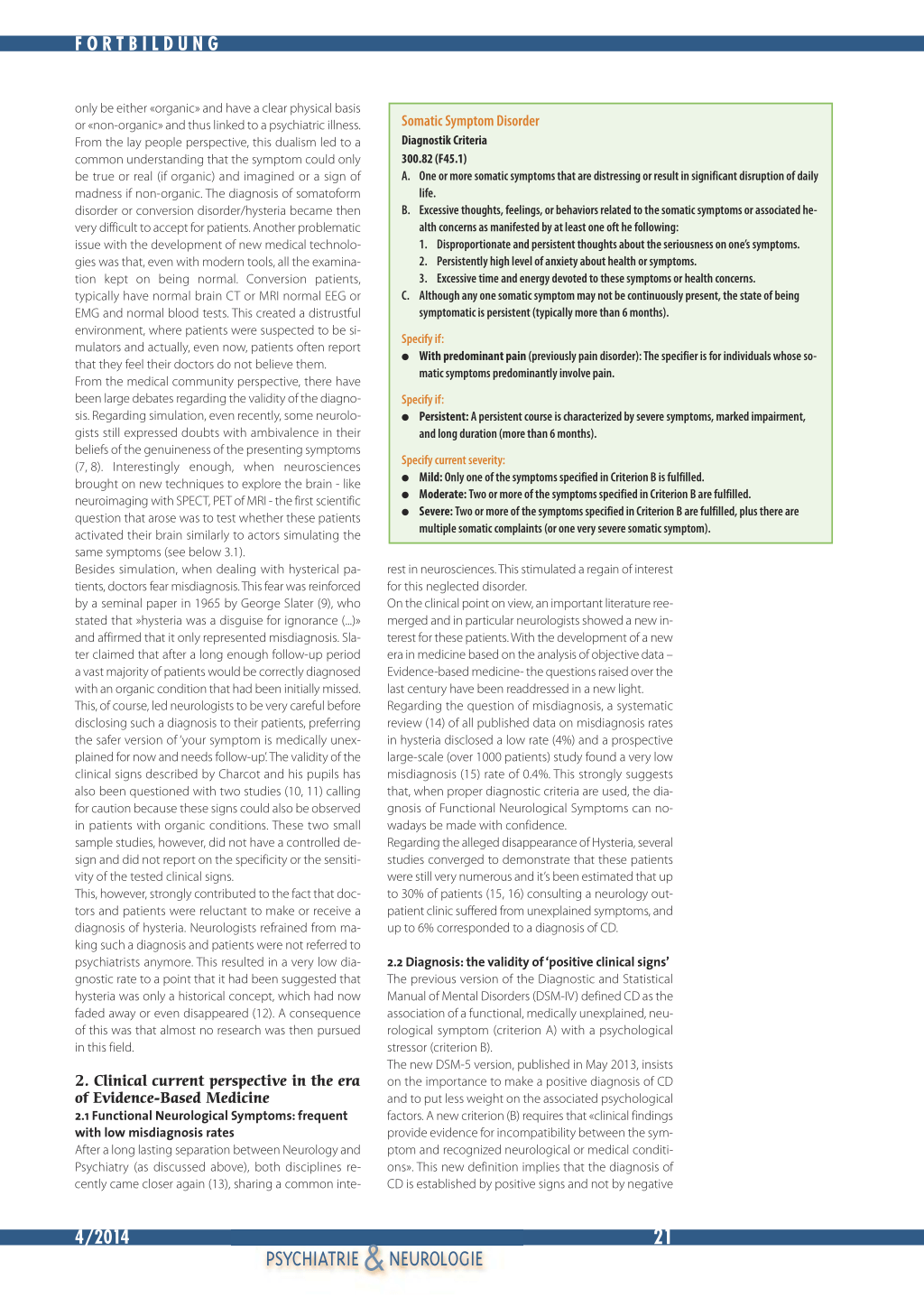
1. Historical Perspective 1. 1 Functional Neurological Symptoms: a debated Terminology In medicine it is not rare to encounter patients who have a medical complaint or symptom for which no disease is found, even after thorough examination. This situation is both distressing for the doctor and the patient because the diagnosis of «medically unexplained symptom» is unsatisfactory. If the symptom persists more than 6 months, it is classified as Somatic Symptom
Glossary CT: computerized tomography MRI: magnetic resonance imaging EEG: electroencephalography EMG: electromyography SPECT: single-photon emission computed
tomography PET: positron emission tomography
Disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM) (1)(see Table 1). If the symptom is neurological in nature (sensory or motor), it is classified as Conversion Disorder (Functional Neurological Symptom disorder), regardless of its duration. Because of the peculiar clinical presentation of neurological symptoms, these have been recognized as early as the Greek Antiquity when Hippocrates (460 BC) suggested the term Hysteria (in Greek hyster = uterus). He indeed observed that the symptoms occurred most often in women and linked the causal mechanism to a dysfunctioning wandering uterus. Over the years, several synonyms have then been employed to designate these neurological symptoms: hysterical, conversive, psychogenic, psychosomatic, dissociative or somatoform. This variety of terms, unfortunately, induces confusion in the medical community even though they do refer to the same clinical entity. There is now a need to use a common unified term and experts have recently advocated for the use of the term «functional» (2) as it is descriptive, non judgmental (3) or stigmatizing and is well accepted by the patients (4).
1. 2 Hysteria: simulation, misdiagnosis or historical concept? Even though the term Hysteria has now disappeared from the medical literature, the stigmatizing and false concepts about this entity still remain. While it is still true that it affects predominantly young women, the role of the uterus has now been replaced by a suspected abnormal brain functioning. Jean-Martin Charcot (1825-1893), the founder of modern Neurology carefully described the clinical presentation and his pupils - like Jean Alexandre Barré and Joseph Babinski further characterized bedside clinical signs typical for hysteria, like the «Arc de Cercle» classically displayed during non-epileptic attacks. Charcot suggested that we might one day have a «big enough microscope» (5) that could enable us to visualize this brain dysfunction. At that time, it was observed that hysterical patients often had previous psychological trauma, mostly childhood sexual abuse. Sigmund Freud, another of Charcot’s pupils, developed then his theory of a psychological trauma being «repressed» and «converted» into a physical symptom (6), hence the term Conversion Disorder (CD). This view fitted with the understanding that our Psyche could influence our body (Soma) and in fact, in the DSM classification, CD is found under the Chapter‘Somatoform Disorder’. However, over the last century, there has been a separation between Neurology and Psychiatry alongside the development of a conceptual view that diseases could
&20 4/2014
PSYCHIATRIE NEUROLOGIE
FORTBILDUNG
only be either «organic» and have a clear physical basis or «non-organic» and thus linked to a psychiatric illness. From the lay people perspective, this dualism led to a common understanding that the symptom could only be true or real (if organic) and imagined or a sign of madness if non-organic. The diagnosis of somatoform disorder or conversion disorder/hysteria became then very difficult to accept for patients. Another problematic issue with the development of new medical technologies was that, even with modern tools, all the examination kept on being normal. Conversion patients, typically have normal brain CT or MRI normal EEG or EMG and normal blood tests. This created a distrustful environment, where patients were suspected to be simulators and actually, even now, patients often report that they feel their doctors do not believe them. From the medical community perspective, there have been large debates regarding the validity of the diagnosis. Regarding simulation, even recently, some neurologists still expressed doubts with ambivalence in their beliefs of the genuineness of the presenting symptoms (7, 8). Interestingly enough, when neurosciences brought on new techniques to explore the brain - like neuroimaging with SPECT, PET of MRI - the first scientific question that arose was to test whether these patients activated their brain similarly to actors simulating the same symptoms (see below 3.1). Besides simulation, when dealing with hysterical patients, doctors fear misdiagnosis. This fear was reinforced by a seminal paper in 1965 by George Slater (9), who stated that »hysteria was a disguise for ignorance (...)» and affirmed that it only represented misdiagnosis. Slater claimed that after a long enough follow-up period a vast majority of patients would be correctly diagnosed with an organic condition that had been initially missed. This, of course, led neurologists to be very careful before disclosing such a diagnosis to their patients, preferring the safer version of ‘your symptom is medically unexplained for now and needs follow-up’. The validity of the clinical signs described by Charcot and his pupils has also been questioned with two studies (10, 11) calling for caution because these signs could also be observed in patients with organic conditions. These two small sample studies, however, did not have a controlled design and did not report on the specificity or the sensitivity of the tested clinical signs. This, however, strongly contributed to the fact that doctors and patients were reluctant to make or receive a diagnosis of hysteria. Neurologists refrained from making such a diagnosis and patients were not referred to psychiatrists anymore. This resulted in a very low diagnostic rate to a point that it had been suggested that hysteria was only a historical concept, which had now faded away or even disappeared (12). A consequence of this was that almost no research was then pursued in this field.
2. Clinical current perspective in the era of Evidence-Based Medicine 2.1 Functional Neurological Symptoms: frequent with low misdiagnosis rates After a long lasting separation between Neurology and Psychiatry (as discussed above), both disciplines recently came closer again (13), sharing a common inte-
Somatic Symptom Disorder
Diagnostik Criteria 300.82 (F45.1) A. One or more somatic symptoms that are distressing or result in significant disruption of daily
life. B. Excessive thoughts, feelings, or behaviors related to the somatic symptoms or associated he-
alth concerns as manifested by at least one oft he following: 1. Disproportionate and persistent thoughts about the seriousness on one’s symptoms. 2. Persistently high level of anxiety about health or symptoms. 3. Excessive time and energy devoted to these symptoms or health concerns. C. Although any one somatic symptom may not be continuously present, the state of being symptomatic is persistent (typically more than 6 months).
Specify if: G With predominant pain (previously pain disorder): The specifier is for individuals whose so-
matic symptoms predominantly involve pain.
Specify if: G Persistent: A persistent course is characterized by severe symptoms, marked impairment,
and long duration (more than 6 months).
Specify current severity: G Mild: Only one of the symptoms specified in Criterion B is fulfilled. G Moderate: Two or more of the symptoms specified in Criterion B are fulfilled. G Severe: Two or more of the symptoms specified in Criterion B are fulfilled, plus there are
multiple somatic complaints (or one very severe somatic symptom).
rest in neurosciences. This stimulated a regain of interest for this neglected disorder. On the clinical point on view, an important literature reemerged and in particular neurologists showed a new interest for these patients. With the development of a new era in medicine based on the analysis of objective data – Evidence-based medicine- the questions raised over the last century have been readdressed in a new light. Regarding the question of misdiagnosis, a systematic review (14) of all published data on misdiagnosis rates in hysteria disclosed a low rate (4%) and a prospective large-scale (over 1000 patients) study found a very low misdiagnosis (15) rate of 0.4%. This strongly suggests that, when proper diagnostic criteria are used, the diagnosis of Functional Neurological Symptoms can nowadays be made with confidence. Regarding the alleged disappearance of Hysteria, several studies converged to demonstrate that these patients were still very numerous and it’s been estimated that up to 30% of patients (15, 16) consulting a neurology outpatient clinic suffered from unexplained symptoms, and up to 6% corresponded to a diagnosis of CD.
2.2 Diagnosis: the validity of ‘positive clinical signs’ The previous version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) defined CD as the association of a functional, medically unexplained, neurological symptom (criterion A) with a psychological stressor (criterion B). The new DSM-5 version, published in May 2013, insists on the importance to make a positive diagnosis of CD and to put less weight on the associated psychological factors. A new criterion (B) requires that «clinical findings provide evidence for incompatibility between the symptom and recognized neurological or medical conditions». This new definition implies that the diagnosis of CD is established by positive signs and not by negative
4/2014
PSYCHIATRIE & NEUROLOGIE
21
FORTBILDUNG
findings and exclusion. There are plenty clinical signs for CD and a recent systematic review (17) demonstrated that 14 of them have been validated for motor, sensory and gait disorders.
Motor signs include: 1) The Hoover’s sign: consists in testing the flexion of he-
althy limb to look for a reflex simultaneous extension movement of the contralateral paretic limb. It is considered positive when there is a weakness of voluntary hip extension while the involuntary hip extension is normal during contralateral hip flexion against resistance. 2) The abductor sign: follows the same principle as the Hoover sign, during the activation of the abductors. 3) The abduction finger sign: when testing the abduction of fingers in the healthy hand, the fifth finger of the affected hand will show a synkinetic abduction movement, in healthy subject and CD patients. This test is only valid in case of complete hand plegia. 4) The Spinal Injuries Center test: the patient lies in bed with the legs passively positioned in flexion. If the paretic leg maintained the flexed posture, the test is considered positive. 5) Give-away weakness: during the muscular testing, the power of the strength quickly «gives away», while the patient is able to produce a reasonable strength without resistance. 6) The co-contraction sign: is characterized by the simultaneous contraction of an antagonist muscle during voluntary contraction of the agonist muscle 7) Variability or inconsistency of motor performance: is defined by discordance in motor testing between two given situations (complete plegia of a limb tested in supine position, but the patient is able to walk out of the room).
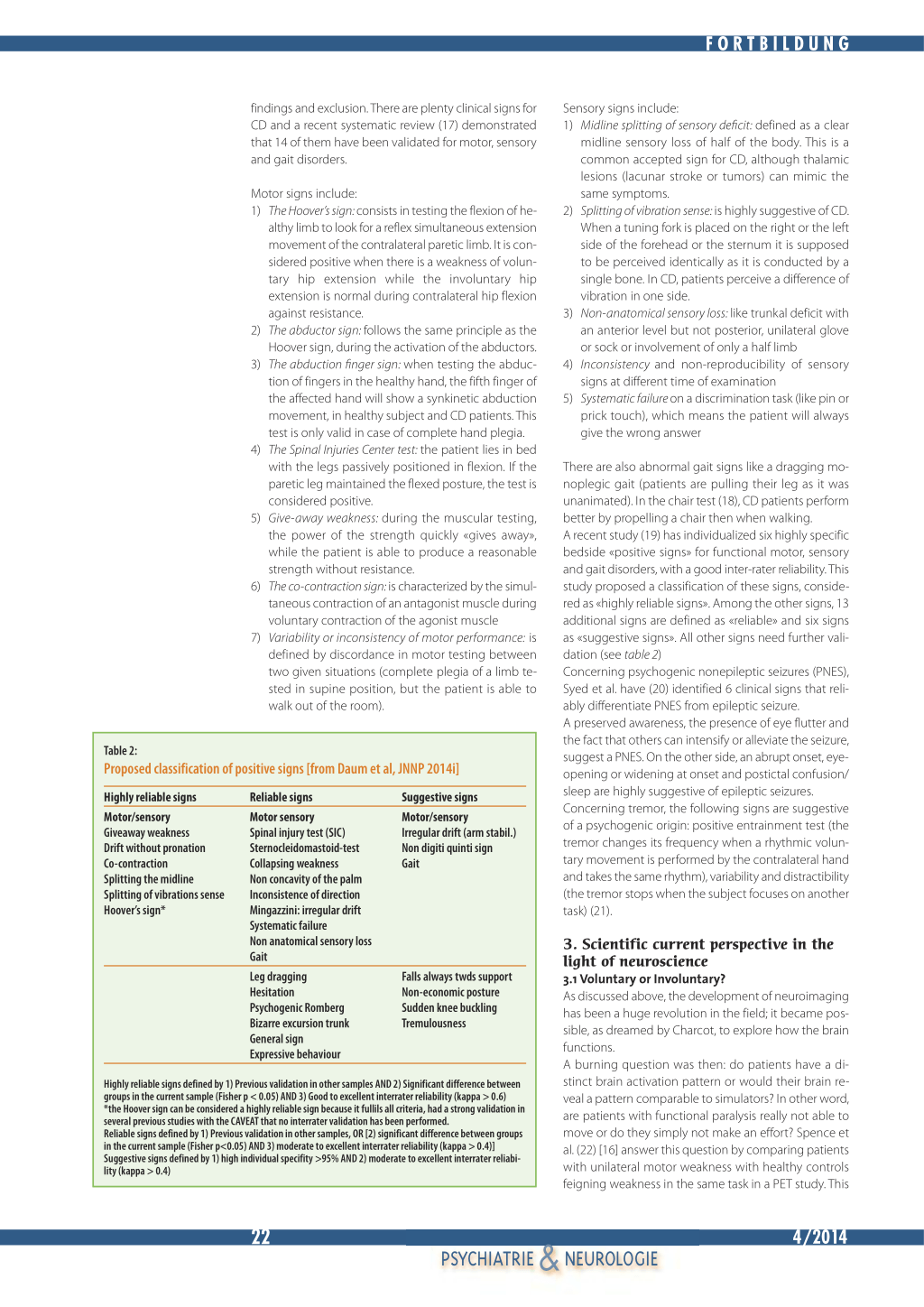
Table 2:
Proposed classification of positive signs [from Daum et al, JNNP 2014i]
Highly reliable signs
Motor/sensory Giveaway weakness Drift without pronation Co-contraction Splitting the midline Splitting of vibrations sense Hoover’s sign*
Reliable signs
Motor sensory Spinal injury test (SIC) Sternocleidomastoid-test Collapsing weakness Non concavity of the palm Inconsistence of direction Mingazzini: irregular drift Systematic failure Non anatomical sensory loss Gait
Leg dragging Hesitation Psychogenic Romberg Bizarre excursion trunk General sign Expressive behaviour
Suggestive signs Motor/sensory Irregular drift (arm stabil.) Non digiti quinti sign Gait
Falls always twds support Non-economic posture Sudden knee buckling Tremulousness
Highly reliable signs defined by 1) Previous validation in other samples AND 2) Significant difference between groups in the current sample (Fisher p < 0.05) AND 3) Good to excellent interrater reliability (kappa > 0.6) *the Hoover sign can be considered a highly reliable sign because it fullils all criteria, had a strong validation in several previous studies with the CAVEAT that no interrater validation has been performed. Reliable signs defined by 1) Previous validation in other samples, OR [2) significant difference between groups in the current sample (Fisher p<0.05) AND 3) moderate to excellent interrater reliability (kappa > 0.4)] Suggestive signs defined by 1) high individual specifity >95% AND 2) moderate to excellent interrater reliability (kappa > 0.4)
Sensory signs include: 1) Midline splitting of sensory deficit: defined as a clear
midline sensory loss of half of the body. This is a common accepted sign for CD, although thalamic lesions (lacunar stroke or tumors) can mimic the same symptoms. 2) Splitting of vibration sense: is highly suggestive of CD. When a tuning fork is placed on the right or the left side of the forehead or the sternum it is supposed to be perceived identically as it is conducted by a single bone. In CD, patients perceive a difference of vibration in one side. 3) Non-anatomical sensory loss: like trunkal deficit with an anterior level but not posterior, unilateral glove or sock or involvement of only a half limb 4) Inconsistency and non-reproducibility of sensory signs at different time of examination 5) Systematic failure on a discrimination task (like pin or prick touch), which means the patient will always give the wrong answer
There are also abnormal gait signs like a dragging monoplegic gait (patients are pulling their leg as it was unanimated). In the chair test (18), CD patients perform better by propelling a chair then when walking. A recent study (19) has individualized six highly specific bedside «positive signs» for functional motor, sensory and gait disorders, with a good inter-rater reliability. This study proposed a classification of these signs, considered as «highly reliable signs». Among the other signs, 13 additional signs are defined as «reliable» and six signs as «suggestive signs». All other signs need further validation (see table 2) Concerning psychogenic nonepileptic seizures (PNES), Syed et al. have (20) identified 6 clinical signs that reliably differentiate PNES from epileptic seizure. A preserved awareness, the presence of eye flutter and the fact that others can intensify or alleviate the seizure, suggest a PNES. On the other side, an abrupt onset, eyeopening or widening at onset and postictal confusion/ sleep are highly suggestive of epileptic seizures. Concerning tremor, the following signs are suggestive of a psychogenic origin: positive entrainment test (the tremor changes its frequency when a rhythmic voluntary movement is performed by the contralateral hand and takes the same rhythm), variability and distractibility (the tremor stops when the subject focuses on another task) (21).
3. Scientific current perspective in the light of neuroscience 3.1 Voluntary or Involuntary? As discussed above, the development of neuroimaging has been a huge revolution in the field; it became possible, as dreamed by Charcot, to explore how the brain functions. A burning question was then: do patients have a distinct brain activation pattern or would their brain reveal a pattern comparable to simulators? In other word, are patients with functional paralysis really not able to move or do they simply not make an effort? Spence et al. (22) [16] answer this question by comparing patients with unilateral motor weakness with healthy controls feigning weakness in the same task in a PET study. This
&22 4/2014
PSYCHIATRIE NEUROLOGIE
FORTBILDUNG
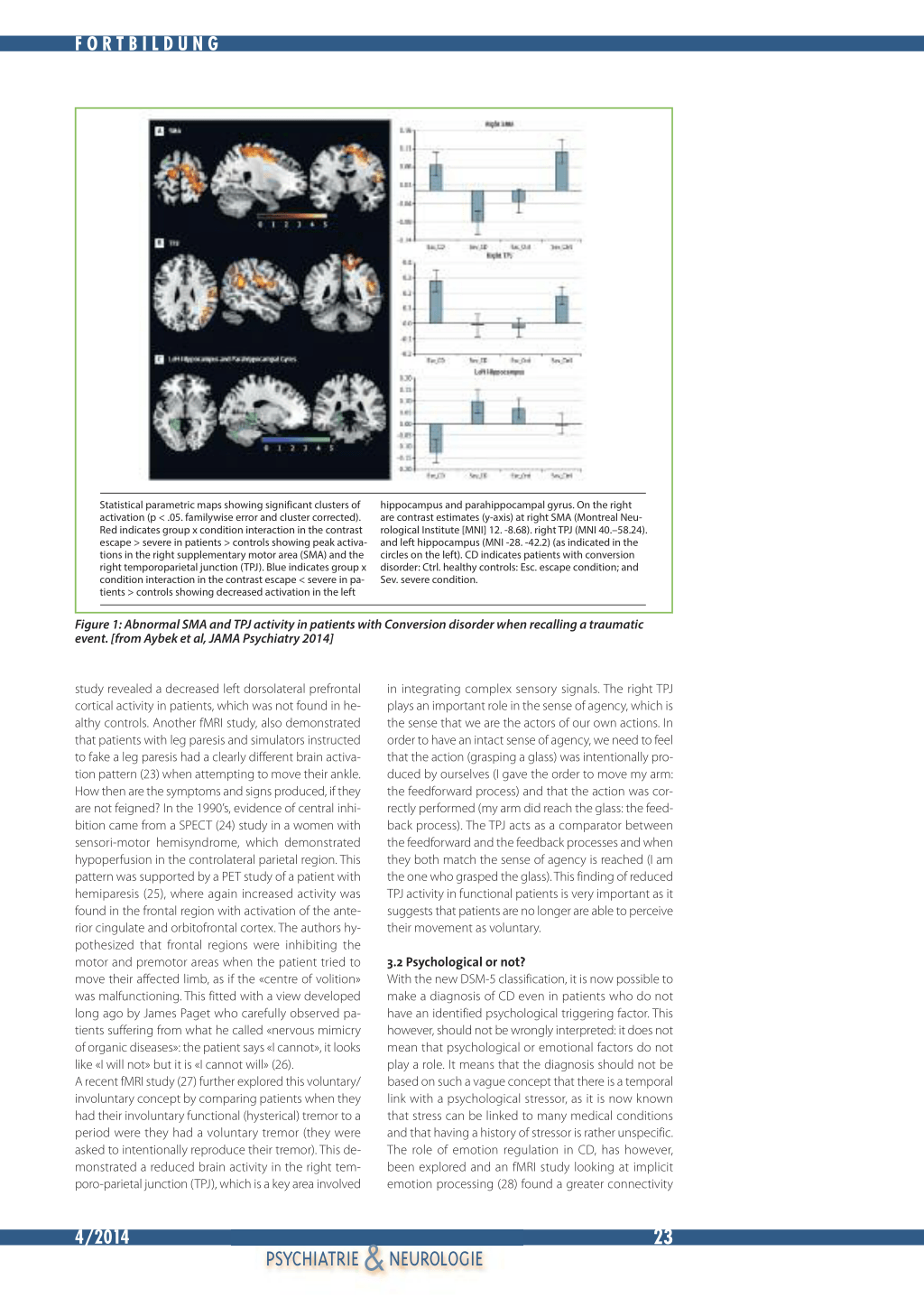
Statistical parametric maps showing significant clusters of activation (p < .05. familywise error and cluster corrected). Red indicates group x condition interaction in the contrast escape > severe in patients > controls showing peak activations in the right supplementary motor area (SMA) and the right temporoparietal junction (TPJ). Blue indicates group x condition interaction in the contrast escape < severe in patients > controls showing decreased activation in the left
hippocampus and parahippocampal gyrus. On the right are contrast estimates (y-axis) at right SMA (Montreal Neurological Institute [MNI] 12. -8.68). right TPJ (MNI 40.–58.24). and left hippocampus (MNI -28. -42.2) (as indicated in the circles on the left). CD indicates patients with conversion disorder: Ctrl. healthy controls: Esc. escape condition; and Sev. severe condition.
Figure 1: Abnormal SMA and TPJ activity in patients with Conversion disorder when recalling a traumatic event. [from Aybek et al, JAMA Psychiatry 2014]
study revealed a decreased left dorsolateral prefrontal cortical activity in patients, which was not found in healthy controls. Another fMRI study, also demonstrated that patients with leg paresis and simulators instructed to fake a leg paresis had a clearly different brain activation pattern (23) when attempting to move their ankle. How then are the symptoms and signs produced, if they are not feigned? In the 1990’s, evidence of central inhibition came from a SPECT (24) study in a women with sensori-motor hemisyndrome, which demonstrated hypoperfusion in the controlateral parietal region. This pattern was supported by a PET study of a patient with hemiparesis (25), where again increased activity was found in the frontal region with activation of the anterior cingulate and orbitofrontal cortex. The authors hypothesized that frontal regions were inhibiting the motor and premotor areas when the patient tried to move their affected limb, as if the «centre of volition» was malfunctioning. This fitted with a view developed long ago by James Paget who carefully observed patients suffering from what he called «nervous mimicry of organic diseases»: the patient says «I cannot», it looks like «I will not» but it is «I cannot will» (26). A recent fMRI study (27) further explored this voluntary/ involuntary concept by comparing patients when they had their involuntary functional (hysterical) tremor to a period were they had a voluntary tremor (they were asked to intentionally reproduce their tremor). This demonstrated a reduced brain activity in the right temporo-parietal junction (TPJ), which is a key area involved
in integrating complex sensory signals. The right TPJ plays an important role in the sense of agency, which is the sense that we are the actors of our own actions. In order to have an intact sense of agency, we need to feel that the action (grasping a glass) was intentionally produced by ourselves (I gave the order to move my arm: the feedforward process) and that the action was correctly performed (my arm did reach the glass: the feedback process). The TPJ acts as a comparator between the feedforward and the feedback processes and when they both match the sense of agency is reached (I am the one who grasped the glass). This finding of reduced TPJ activity in functional patients is very important as it suggests that patients are no longer are able to perceive their movement as voluntary.
3.2 Psychological or not? With the new DSM-5 classification, it is now possible to make a diagnosis of CD even in patients who do not have an identified psychological triggering factor. This however, should not be wrongly interpreted: it does not mean that psychological or emotional factors do not play a role. It means that the diagnosis should not be based on such a vague concept that there is a temporal link with a psychological stressor, as it is now known that stress can be linked to many medical conditions and that having a history of stressor is rather unspecific. The role of emotion regulation in CD, has however, been explored and an fMRI study looking at implicit emotion processing (28) found a greater connectivity
4/2014
PSYCHIATRIE & NEUROLOGIE
23
FORTBILDUNG
in CD patients between the amygdala- a key region for emotion regulation- and the supplementary motor area (SMA)- a key region in motor planning, suggesting an aberrant limbic-motor network in this disorder. Another study looked at more specific emotion regulation in a task where patients were asked to recall a traumatic event from their own life (29). This showed again the same amygdala-SMA enhanced connectivity in patients. An additional finding of that study was, that when patient had to recall the trauma, they displayed an increased dorsolateral prefrontal cortex activity and concomitant reduced hippocampal activity which is a pattern known to be involved in active forgetting of unwanted memories (30). This suggests that, as postulated by Freud, in CD patients, recalling of a traumatic event was «fought» or «repressed» by the subject. This was accompanied by an abnormal activity in both the SMA and the TPJ (see Figure 1), the two regions already shown to play a role in the production of functional symptoms. Altogether, this study suggests that the «repression» of the traumatic memory is accompanied by an effect on motor planning (SMA) and sense of agency (TPJ), which could correspond to what Freud called a »conversion» process.
4. Treatment In the recent decades there has been a lot of effort to conduct studies to formally test the efficacy of several approaches. When there is no proof of efficacy for hypnosis (31), transcranial stimulation (32) or drugs (33), there is evidence for the efficacy of different psychotherapeutic approaches. Tailored psychotherapy (34), cognitive behavioral therapy (35) and self-help cognitive therapy (36) can be effective. Concerning non-epileptic seizures, there might be some benefit from antidepressant drugs (37). A very recent large-scale study confirmed the efficacy of psychotherapy (38) for nonepileptic seizures (with or without drug) and this should be systematically recommended to patients. For motor conversion patients, physiotherapy has been shown to be effective (39). Overall, the practical recommendation nowadays for the care of CD patients is a multi-steps plan. The first step lies in a thorough and careful examination in order to make a proper diagnosis with positive evidence. The second step is to communicate the diagnosis to the patient by telling him what he has and not only what he does not have. Indeed many doctors still announce a list of diagnosis they excluded such as tumor, multiple sclerosis, stroke etc... but do not give the patient a name of the diagnosis they have. This is where the term functional is useful and it can be helpful also to direct patient to a website providing medical information on that disorder (www.neurosymptoms.org). The third step is to make a good alliance with the patient allowing referring them to a psychiatrist without giving the patient the impression they are «mad» or «imagine their symptoms» and without giving them the impression the neurologist abandons his/her patient. This can be overcome by a common follow-up between both the neurologist and the psychiatrist (40). The psychiatric evaluation is important, as many CD patients also suffer from psychiatric co-morbidities such as anxiety and/or depression, which need to be treated. Then the psych-
iatric referral can also allow proposing a more thorough psychotherapeutic treatment to some patients. The final and ideal step is to have a multidisciplinary (41) approach involving the general practitioner, the neurologist, the psychiatrist and when relevant the physiotherapist, speech, therapist, social worker and nurses. In the future, the development of specialized centers, with in-patients and outpatients treatment plans, should be a priority for these complex patients.
5. Conclusion Hysteria still exists even though this term has been replaced by less stigmatizing ones such as: psychogenic disorder, dissociative disorder, conversion disorder and in the future the unified term will be Functional Neurological Symptom. The fact that the diagnosis can be difficult to establish in some situation highlights the importance of positive signs rather than negative findings. With the validation of many of these bedside signs, doctors should now be confidant in making their diagnosis and in clearly communicating this diagnosis to their patients. This is reinforced by studies proving that there is a low misdiagnosis rate. The etiology is still to be determined but stressful life events are suspected to play a role in the cerebral dysfunction. Even if there is no efficient treatment yet, a multidisciplinary approach involving both a neurologist and a psychiatrist seems to improve the prognosis of these patients. G
Adresse: Dr Selma Aybek
Chefärztin Neurologie – HUG Rue Gabrielle-Perret-Gentil 4
1205 Genève
Maître-assistante Neurosciences Fondamentales - UNIGE Laboratory for Behavioral Neurology and Imaging
of Cognition bureau7008 – CMU Rue Michel-Servet 1, 1211 Genève Mail:Selma.Aybek@unige.ch
1 Service de Neurologie, DNC, Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne, Switzerland
2 Service de Neurologie, DNC, Hôpitaux Universitaire Genevois (HUG), Genève, Switzerland
References: 1. APA. Diagnostic and statistical manual of mental disorders: DSM-IV.
Washington DC: American Psychiatric Association, 1994. 2. Carson AJ, Brown R, David AS, et al. Functional (conversion) neuro-
logical symptoms: research since the millennium. J Neurol Neurosurg Psychiatry 2012; 83: 842–850. 3. Kanaan RA, Armstrong D, Wessely SC. The function of ‘functional’: a mixed methods investigation. J Neurol Neurosurg Psychiatry 2012; 83: 248–250. 4. Stone J, Wojcik W, Durrance D, et al. What should we say to patients with symptoms unexplained by disease? The «number needed to offend». Bmj 2002; 325: 1449–1450. 5. Charcot J. Clinical Lectures on diseases of the nervous system. London: New Sydenham Society, 1889. 6. Breuer J FS. Studies in Hysteria. . The standard edition of the complete psychological works of Sigmund Freud, vol II. London: Hogarth Press, 1895. 7. Kanaan RA, Armstrong D, Wessely SC. Neurologists’ understanding and management of conversion disorder. J Neurol Neurosurg Psychiatry 2011; 82: 961–966. 8. Kanaan R, Armstrong D, Barnes P, Wessely S. In the psychiatrist’s chair: how neurologists understand conversion disorder. Brain 2009; 132: 2889–2896. 9. Slater ET, Glithero E. A follow-up of patients diagnosed as suffering from «hysteria». J Psychosom Res 1965; 9: 9–13.
&24 4/2014
PSYCHIATRIE NEUROLOGIE
FORTBILDUNG
10. Gould R, Miller BL, Goldberg MA, Benson DF. The validity of hysterical signs and symptoms. J Nerv Ment Dis 1986; 174: 593–597.
11. Chabrol H, Peresson G, Clanet M. Lack of specificity of the traditional criteria for conversion disorders. Eur Psychiatry 1995; 10: 317–319.
12. Stone J, Hewett R, Carson A, Warlow C, Sharpe M. The‘disappearance’ of hysteria: historical mystery or illusion? J R Soc Med 2008; 101: 12–18.
13. Carson AJ. Introducing a ‘neuropsychiatry’ special issue: but what does that mean? J Neurol Neurosurg Psychiatry 2014; 85: 121–122.
14. Stone J, Smyth R, Carson A, et al. Systematic review of misdiagnosis of conversion symptoms and «hysteria». Bmj 2005; 331: 989.
15. Stone J, Carson A, Duncan R, et al. Symptoms ‘unexplained by organic disease’ in 1144 new neurology out-patients: how often does the diagnosis change at follow-up? Brain 2009; 132: 2878–2888.
16. Carson AJ, Ringbauer B, Stone J, McKenzie L, Warlow C, Sharpe M. Do medically unexplained symptoms matter? A prospective cohort study of 300 new referrals to neurology outpatient clinics. J Neurol Neurosurg Psychiatry 2000; 68: 207–210.
17. Daum C, Hubschmid M, Aybek S. The value of ‘positive’ clinical signs for weakness, sensory and gait disorders in conversion disorder: a systematic and narrative review. J Neurol Neurosurg Psychiatry 2014; 85: 180–190.
18. Okun MS, Rodriguez RL, Foote KD, Fernandez HH. The «chair test» to aid in the diagnosis of psychogenic gait disorders. Neurologist 2007; 13: 87–91.
19. Daum C, Gheorghita F, Spatola M, et al. Interobserver agreement and validity of bedside ‘positive signs’ for functional weakness, sensory and gait disorders in conversion disorder: a pilot study. J Neurol Neurosurg Psychiatry 2014.
20. Syed TU, LaFrance WC, Jr., Kahriman ES, et al. Can semiology predict psychogenic nonepileptic seizures? A prospective study. Ann Neurol 2011; 69: 997–1004.
21. Kenney C, Diamond A, Mejia N, Davidson A, Hunter C, Jankovic J. Distinguishing psychogenic and essential tremor. J Neurol Sci 2007; 263: 94–99.
22. Spence SA, Crimlisk HL, Cope H, Ron MA, Grasby PM. Discrete neurophysiological correlates in prefrontal cortex during hysterical and feigned disorder of movement. Lancet 2000; 355: 1243–1244.
23. Stone J, Zeman A, Simonotto E, et al. FMRI in patients with motor conversion symptoms and controls with simulated weakness. Psychosom Med 2007; 69: 961–969.
24. Tiihonen J, Kuikka J, Viinamaki H, Lehtonen J, Partanen J. Altered cerebral blood flow during hysterical paresthesia. Biol Psychiatry 1995; 37: 134–135.
25. John C. Marshalla,*, Peter W. Halliganb, Gereon R. Finkc, Derick T. Wadeb, Richard S.J. Frackowiakc: The functional anatomy of a hysterical paralysis. Cognition 64 (1997) B1–B8.
26. Paget J. Clinical lectures on the nervous mimicry of organic diseases. The Lancet 1873.
27. Voon V, Gallea C, Hattori N, Bruno M, Ekanayake V, Hallett M. The involuntary nature of conversion disorder. Neurology 2010; 74: 223–228.
28. Voon V, Brezing C, Gallea C, et al. Emotional stimuli and motor conversion disorder. Brain 2010; 133: 1526–1536.
29. Aybek S, Nicholson TR, Zelaya F, et al. Neural correlates of recall of life events in conversion disorder. JAMA Psychiatry 2014; 71: 52–60.
30. Anderson MC, Ochsner KN, Kuhl B, et al. Neural systems underlying the suppression of unwanted memories. Science 2004; 303: 232–235.
31. Moene FC, Spinhoven P, Hoogduin KA, van Dyck R. A randomized controlled clinical trial of a hypnosis-based treatment for patients with conversion disorder, motor type. Int J Clin Exp Hypn 2003; 51: 29–50.
32. Pollak TA, Nicholson TR, Edwards MJ, David AS. A systematic review of transcranial magnetic stimulation in the treatment of functional (conversion) neurological symptoms. J Neurol Neurosurg Psychiatry 2014; 85: 191–197.
33. Voon V, Lang AE. Antidepressant treatment outcomes of psychogenic movement disorder. J Clin Psychiatry 2005; 66: 1529–1534.
34. Reuber M, Burness C, Howlett S, Brazier J, Grunewald R. Tailored psychotherapy for patients with functional neurological symptoms: a pilot study. J Psychosom Res 2007; 63: 625–632.
35. Goldstein LH, Chalder T, Chigwedere C, et al. Cognitive-behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology 2010; 74: 1986–1994.
36. Sharpe M, Walker J, Williams C, et al. Guided self-help for functional (psychogenic) symptoms: a randomized controlled efficacy trial. Neurology 2011; 77: 564–572.
37. LaFrance WC, Jr., Keitner GI, Papandonatos GD, et al. Pilot pharmacologic randomized controlled trial for psychogenic nonepileptic seizures. Neurology 2010; 75: 1166–1173.
38. LaFrance WC, Jr., Baird GL, Barry JJ, et al. Multicenter Pilot Treatment Trial for Psychogenic Nonepileptic Seizures: A Randomized Clinical Trial. JAMA Psychiatry 2014.
39. Nielsen G, Stone J, Edwards MJ. Physiotherapy for functional (psychogenic) motor symptoms: a systematic review. J Psychosom Res 2013; 75: 93–102.
40. Aybek S HM, Mossinger C , Berney A , Vingerhoets F Early intervention for conversion disorder: neurologists and psychiatrists working together. Acta Neuropsychiatrica 2013; 25.
41. Saifee TA, Kassavetis P, Parees I, et al. Inpatient treatment of functional motor symptoms: a long-term follow-up study. J Neurol 2012.