
Transkript
FORTBILDUNG
Sexually transmitted diseases
Malignant syphilis in an HIV infected female patient
AHMAD JALILI1+2
1 Dermatology & Skin Care, Bürgenstock Medical Center, Obbürgen 2 PsoriNet Switzerland
Introduction
Syphilis is a sexually transmitted disease by the spirochetal bacterium Treponema pallidum. The route of transmission of syphilis is almost always sexual contact, although there are examples of congenital syphilis via transmission from mother to child in utero (1). The course of disease is composed of primary, secondary, latent, tertiary and neurosyphilis (2). Primary syphilis occurs approximately 10–90 days after the initial exposure (average 21 days). A skin lesion (chancre) appears at the point of contact, which is usually the genital organs, but can be anywhere on the body. The lesion may persist for 4 to 6 weeks and usually heals spontaneously. Local lymph node swelling can occur. During this stage individuals are otherwise asymptomatic 2). Typical presentation of secondary syphilis usually includes localized or diffuse symmetric mucocutaneous lesions and generalized non-tender lymphadenopathy. Initial lesions are bilaterally symmetric, pale red to pink, discrete, round macules that measure 5–10 mm in diameter and are distributed on the trunk, proximal extremities, palms and soles. Tiny papular follicular syphilids involving hair follicles may result in patchy alopecia. In a small percentage of patients, highly infectious papules develop at the mucocutaneous junctions and, in moist intertriginous skin, become hypertrophic and dull pink or gray (condyloma lata). A patient with syphilis is most contagious when he or she has secondary syphilis. Other symptoms common at this stage include fever, sore throat, malaise, weight loss, headache and meningismus (2). Latent syphilis is defined as having serologic proof of infection without signs or symptoms of disease. Latent syphilis is further described as either early (defined as having syphilis for one year) or late (having syphilis for more than a year). The distinction is important for both therapy and risk for transmission. In most cases, the time point of infection is often not known and should be presumed to be late for the purpose of therapy. Early latent syphilis may be treated with a single intramuscular (i.m.) injection of a long-acting penicillin. Late latent syphilis requires three weekly injections (3).
Tertiary syphilis usually occurs 1–10 years after the initial infection, however in some cases it can take up to 50 years. This stage is characterized by the formation of gummas, which are soft, tumor-like balls of inflammation known as granulomas. The granulomas are chronic and represent an inability of the immune system to completely clear the organism. They may appear almost anywhere in the body including in the bones (4). Neurosyphilis refers to a site of infection involving the central nervous system (CNS). It may occur at any stage of syphilis. Neurosyphilis is now most common in patients with HIV infection. Approximately 35 to 40 percent of persons with secondary syphilis have asymptomatic central nervous system (CNS) involvement, as demonstrated by an abnormal leukocyte cell count, protein level, glucose level or reactivity to Venereal Disease Research Laboratory (VDRL) antibody test in cerebrospinal fluid (CSF) examination (5). Malignant syphilis or lues maligna is a rare manifestation of secondary syphilis. It is characterized by papulopustular skin lesions that rapidly enlarge and evolve into round or oval ulcers with sharp borders, centrally covered by a dark, rupioid crust. The diagnosis is usually established by strongly positive serological tests, a severe Jarisch-Herxheimer reaction, and an excellent response to antibiotic therapy (3). Here we report a case of malignant syphilis in a HIV positive patient with spectacular clinical presentation where despite previous unsuccessful therapy with cephalosporin and lack of spirochets in dark field microscopy, we could establish the diagnosis with the help of histopathology and syphilis serology and successfully and rapidly treat with penicillin.
Case report
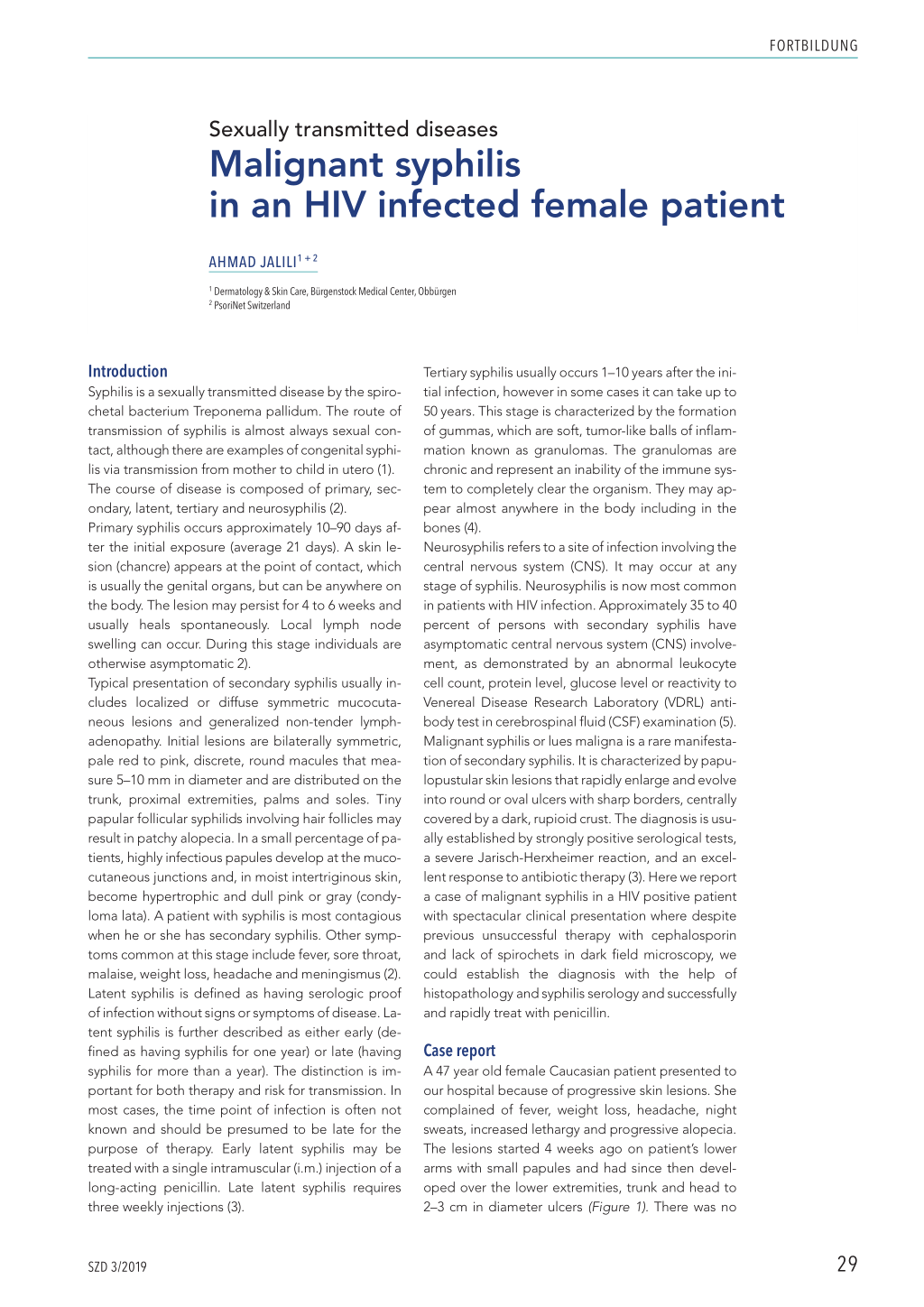
A 47 year old female Caucasian patient presented to our hospital because of progressive skin lesions. She complained of fever, weight loss, headache, night sweats, increased lethargy and progressive alopecia. The lesions started 4 weeks ago on patient’s lower arms with small papules and had since then developed over the lower extremities, trunk and head to 2–3 cm in diameter ulcers (Figure 1). There was no
SZD 3/2019
29
FORTBILDUNG
Figure 1. Clinical presentation of the patient at the time of admission. Painless, non-pruritic, partially rupioid-crusted ulcerative skin lesions starting with small papules.
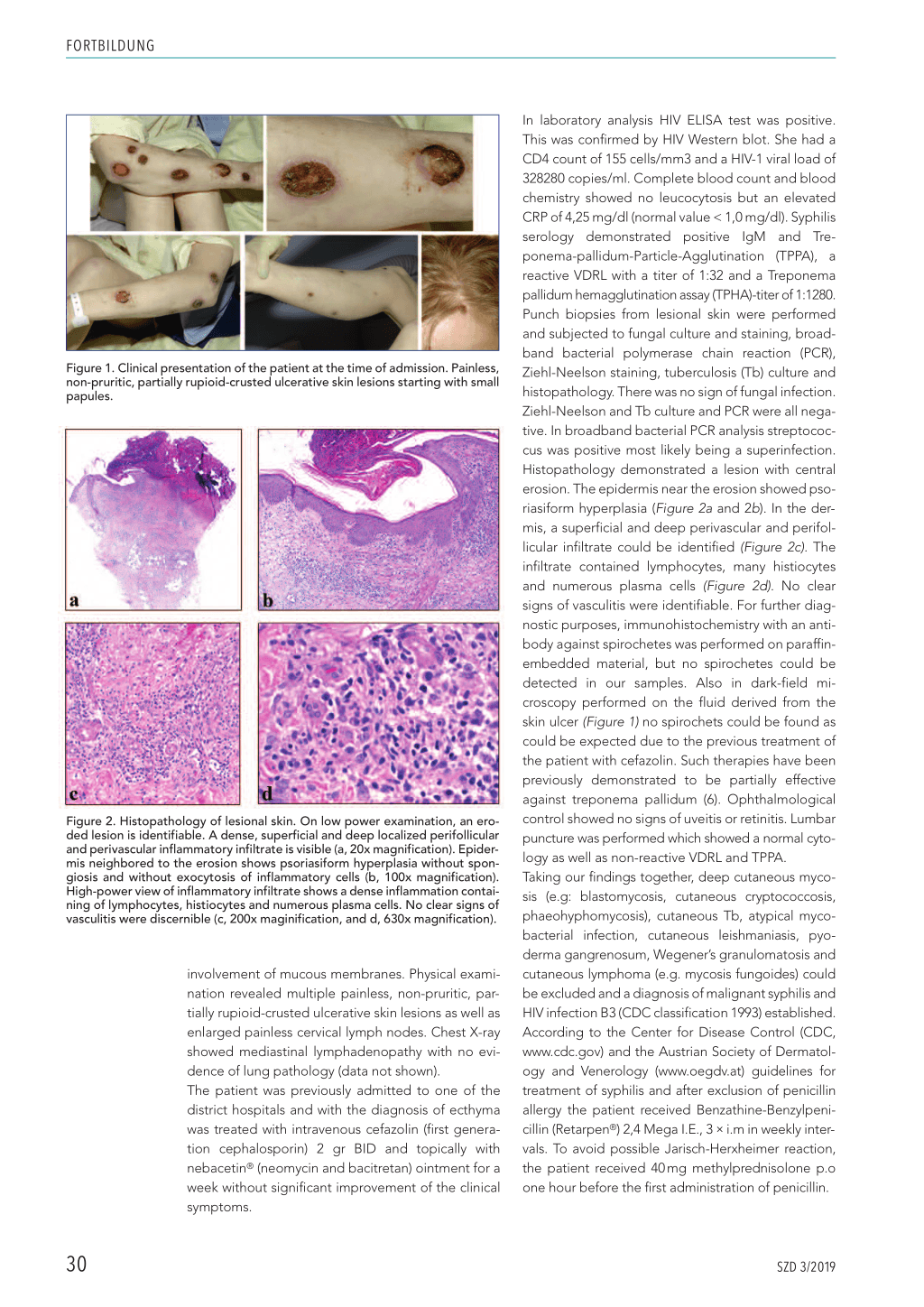
Figure 2. Histopathology of lesional skin. On low power examination, an eroded lesion is identifiable. A dense, superficial and deep localized perifollicular and perivascular inflammatory infiltrate is visible (a, 20x magnification). Epidermis neighbored to the erosion shows psoriasiform hyperplasia without spongiosis and without exocytosis of inflammatory cells (b, 100x magnification). High-power view of inflammatory infiltrate shows a dense inflammation containing of lymphocytes, histiocytes and numerous plasma cells. No clear signs of vasculitis were discernible (c, 200x maginification, and d, 630x magnification).
involvement of mucous membranes. Physical examination revealed multiple painless, non-pruritic, partially rupioid-crusted ulcerative skin lesions as well as enlarged painless cervical lymph nodes. Chest X-ray showed mediastinal lymphadenopathy with no evidence of lung pathology (data not shown). The patient was previously admitted to one of the district hospitals and with the diagnosis of ecthyma was treated with intravenous cefazolin (first generation cephalosporin) 2 gr BID and topically with nebacetin® (neomycin and bacitretan) ointment for a week without significant improvement of the clinical symptoms.
In laboratory analysis HIV ELISA test was positive. This was confirmed by HIV Western blot. She had a CD4 count of 155 cells/mm3 and a HIV-1 viral load of 328280 copies/ml. Complete blood count and blood chemistry showed no leucocytosis but an elevated CRP of 4,25 mg/dl (normal value < 1,0 mg/dl). Syphilis serology demonstrated positive IgM and Treponema-pallidum-Particle-Agglutination (TPPA), a reactive VDRL with a titer of 1:32 and a Treponema pallidum hemagglutination assay (TPHA)-titer of 1:1280. Punch biopsies from lesional skin were performed and subjected to fungal culture and staining, broadband bacterial polymerase chain reaction (PCR), Ziehl-Neelson staining, tuberculosis (Tb) culture and histopathology. There was no sign of fungal infection. Ziehl-Neelson and Tb culture and PCR were all negative. In broadband bacterial PCR analysis streptococcus was positive most likely being a superinfection. Histopathology demonstrated a lesion with central erosion. The epidermis near the erosion showed psoriasiform hyperplasia (Figure 2a and 2b). In the dermis, a superficial and deep perivascular and perifollicular infiltrate could be identified (Figure 2c). The infiltrate contained lymphocytes, many histiocytes and numerous plasma cells (Figure 2d). No clear signs of vasculitis were identifiable. For further diagnostic purposes, immunohistochemistry with an antibody against spirochetes was performed on paraffinembedded material, but no spirochetes could be detected in our samples. Also in dark-field microscopy performed on the fluid derived from the skin ulcer (Figure 1) no spirochets could be found as could be expected due to the previous treatment of the patient with cefazolin. Such therapies have been previously demonstrated to be partially effective against treponema pallidum (6). Ophthalmological control showed no signs of uveitis or retinitis. Lumbar puncture was performed which showed a normal cytology as well as non-reactive VDRL and TPPA. Taking our findings together, deep cutaneous mycosis (e.g: blastomycosis, cutaneous cryptococcosis, phaeohyphomycosis), cutaneous Tb, atypical mycobacterial infection, cutaneous leishmaniasis, pyoderma gangrenosum, Wegener’s granulomatosis and cutaneous lymphoma (e.g. mycosis fungoides) could be excluded and a diagnosis of malignant syphilis and HIV infection B3 (CDC classification 1993) established. According to the Center for Disease Control (CDC, www.cdc.gov) and the Austrian Society of Dermatology and Venerology (www.oegdv.at) guidelines for treatment of syphilis and after exclusion of penicillin allergy the patient received Benzathine-Benzylpenicillin (Retarpen®) 2,4 Mega I.E., 3 i.m in weekly intervals. To avoid possible Jarisch-Herxheimer reaction, the patient received 40 mg methylprednisolone p.o one hour before the first administration of penicillin. 30 SZD 3/2019 FORTBILDUNG The therapy was accompanied with complete regression of the skin lesions (Figure 3) and a 4 fold decrease in VDRL titer over a period of four weeks. Discussion The clinical manifestations of secondary syphilis vary greatly. Skin lesions are often generalized, but localized lesions can occur. In HIV-infected patients, the course of syphilis can be atypical (7). The characteristics of malignant syphilis has been defined by Neisser in 1897 (8). The onset of disease is characterized by prodrome which is composed of arthralgia, malaise and fever. Skin lesions start as papules and evolve into pustules, followed by necrosis of the center of the lesion. Despite the name malignant, malignant syphilis usually responds very well and rapidly to proper therapy (6). So far vast majority of published cases of malignant syphilis are in HIV positive patients. But cases in diabetic, malnourished as well as HIV negative patients have been also documented (9, 10). Unfortunately, there are no exact data on the incidence of malignant syphilis among HIV positive patients but a single report by Schöfer H. et al. in 1996 shows incidence of malignant syphilis to be about 7.3% in 151 active syphilis cases diagnosed Figure 3. Clinical presentation of the patient at the time of admission and 4 weeks after start of the treatment with Benzathine-Benzylpenicillin (Retarpen®) 2,4 Mega I.E., 3x i.m in weekly intervals. in a population of 11 368 HIV positive patients (11). Diagnosis of malignant syphilis is based on the clinical presentation of the disease, dark-field microscopy performed on the fluid obtained from the lesional skin, syphilis serology and histopathology looking for the presence of spirochetes (using specific antibodies) as well as presence of lymphocytic infiltrates among others plasma cells in the dermis. In the case of our patient because of previous therapy with cefazolin we were not able to identify spirochetes in dark- SZD 3/2019 31 FORTBILDUNG field microscopy but syphilis serology was highly pos- itive and the histopathology was compatible typically with numerous plasma cell infiltrates in the dermis. It is worth mentioning that syphilis serology can be negative in HIV positive patients (12). As has been previously described in literature our patient also re- sponded very quickly to the antibiotic therapy with Benzathine-Benzylpenicillin. Finally we would like to mention that malignant syphilis should be kept in mind when dealing with HIV positive patients having skin ul- cers and that the therapy has to be started as soon as possible unless other diagnoses are evident. L Ahmad Jalili M.D, Ph.D Dermatology & Skin Care Bürgenstock Medical Center Bürgenstock 30, 6363 Obbürgen Tel: 041 612 66 60, Fax: 041 612 66 61 E-Mail: ahmad.jalili@buergenstock.ch Abbildungen: Ahmad Jalili References 1. Simms I, Broutet N (2008) Congenital syphilis re-emerging. J Dtsch Dermatol Ges 6: 269–272. 2. Peeling RW, Hook EW, 3rd (2006) The pathogenesis of syphilis: the Great Mim- icker, revisited. J Pathol 208: 224–232. 3. Dourmishev LA, Dourmishev AL (2005) Syphilis: uncommon presentations in adults. Clin Dermatol 23: 555–564. 4. Augenbraun M (2000) Treatment of latent and tertiary syphilis. Hosp Pract (Min- neap) 35: 89–95; quiz 96. 5. Delli FS, Mourellou O, Chaidemenos G, Anagnostou E, Amaxopoulos K (2007) Neurosyphilis: a reality again. J Eur Acad Dermatol Venereol 21: 398–399. 6. Stoner BP (2007) Current controversies in the management of adult syphilis. Clin Infect Dis 44 Suppl 3: S130–146. 7. Zetola NM, Klausner JD (2007) Syphilis and HIV infection: an update. Clin Infect Dis 44: 1222–1228. 8. Neisser (1897) Malignant syphilis. Br J Dermatol 9: 11–26. 9. Hofmann UB, Hund M, Brocker EB, Hamm H (2005) [«Lues maligna» in a female patient with diabetes]. J Dtsch Dermatol Ges 3: 780–782. 10. Williams J, Veluchamy V, Sundararaj AS (1994) Rupial syphilides in a single male. Int J STD AIDS 5: 67–68. 11. Schofer H, Imhof M, Thoma-Greber E, Brockmeyer NH, Hartmann M, Gerken G et al. (1996) Active syphilis in HIV infection: a multicentre retrospective survey. The German AIDS Study Group (GASG). Genitourin Med 72:176–181. 12. Farhi D, Benhaddou N, Grange P, Zizi N, Deleuze J, Morini JP, et al. (2009) Clinical and serologic baseline and follow-up features of syphilis according to HIV status in the post-HAART era. Medicine (Baltimore) 88: 331–340. 32 SZD 3/2019