
Transkript
CONGRESS-HANDOUT
SGML
Stress Urinary Incontinence and Laser Therapy
BY AnA MitroviĆ JovAnoviĆ
Genuine stress incontinence is the most common form of urinary incontinence. Stress urinary incontinence (SUI) is defined as involuntary urine loss that is provoked by an increase in intra-abdominal pressure, usually during physical activity and upon coughing sneezing, laughing or when engaging in intercourse. Factors that increase risk of SUI are childbirth, age, obesity, chronic constipation and heavy lifting (1). Vaginal and urethral epithelia originate from the same embyologic tissue and are both estrogen dependent and subject to the negative effects of estrogen deprivation. One of the contributing factors to stress incontinence in menopausal women is loss of the para-urethral vascular plexus that surrounds the proximal urethra. In a premenopausal state, this lush network of vessels serves as a «hydraulic sphincter» to augment other continence mechanisms. In a postmenopausal state, however, the vascular plexus becomes flat and ineffective (2). The vagina is a fibro-muscular and tubular part of the female genital tract, which extends from the outer genitals (the vulva) up to the cervix and the uterus. The anterior surface of the vagina is connected to the fundus of the bladder and the urethra. However, the posterior surface is separated from the rectum. Urinary incontinence affects 200 million people worldwide. A large meta-analysis reported an estimated prevalence for urinary incontinence in women aged 30 to 60 years of 30 percent, with approximately half of the cases attributed to SUI (15%). On average, women will wait 6.5 years after having experienced symptoms for the first time before they obtain their bladder control problem(s). Bladder control problems also affect younger people, especially women who have just given birth. In fact, one in four women over 18 years experiences episodes of leaking urine involuntarily. Even mild symptoms affect social, sexual, interpersonal and professional function. Tests for a cystoceles include a pelvic exam and urodynamics, a group of tests developed to evaluate bladder function (1, 2, 3). Genitourinary syndrome of menopause (GSM) has a significant impact on the tropism of the genital and lower urinary tracts and can considerably impair sexual function. Fractional CO2 lasers, however, have a regenerative effect on vulvovaginal tissue tropism after menopause. Effects of the pixel CO2 laser fractional technology create micro-ablation and thermal
damage to the mucosa and sub-mucosa causing the neocollagenesis, and remodelling of the connective tissue of the lamina propria is achieved in response to the controlled injury caused by the deep thermal effect. CO2 laser effects are: L Contracts existing collagen and elastin fibers and
stimulates the formation of new collagen fibers, which may lead to vaginal tightening and mid urethra support strengthening. L Neovascularization and improved vaginal lubrication. Normalizes vaginal flora and pH and helps to eliminate chronic vaginal infections. L Restores the mucosal quality of the vaginal walls and enhances the sensitivity of vaginal tissue. L Treats the entire pre-urethral space, increasing the thickness of the vaginal walls and providing better support to the mid urethra underside.
Ana Mitrović Jovanović
The studies suggest that intravaginal fractional CO2laser therapy for postmenopausal women with clinical signs and symptoms of GSM and SUI may be effective in improving both vaginal pathophysiology and reported symptoms (4, 5, 6, 7, 8, 9, 10, 11).
Own experience
The aim of the study was to assess the effects of fractional pixel CO2 laser therapy on the symptoms of stress urinary incontinence.
Results
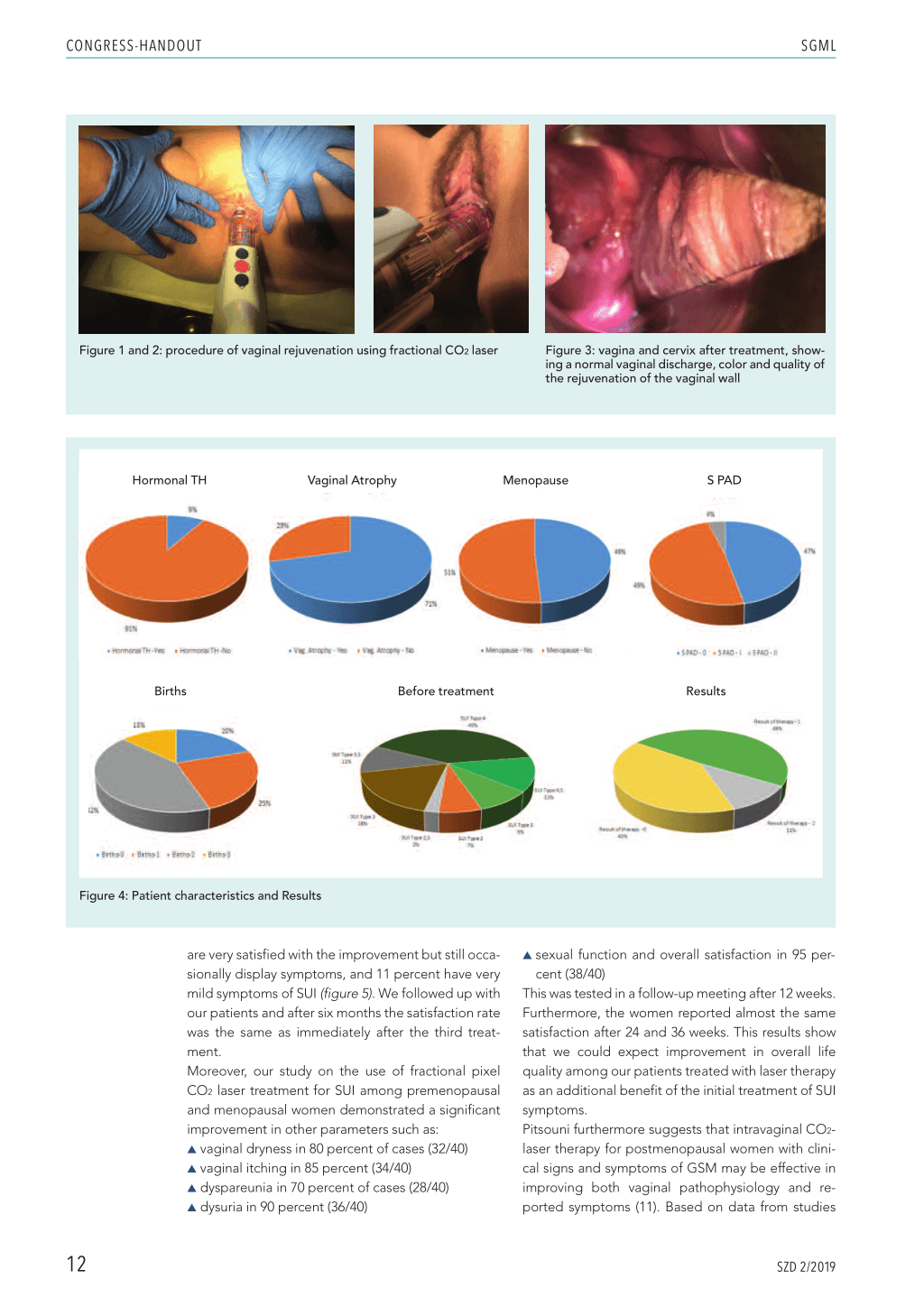
We evaluated 45 premenopausal and menopausal women with SUI problems. Among our patients, 51 percent were menopausal and 49 percent were premenopausal. All of them had symptoms of SUI but almost half of them, 47 percent, had no pathology of the vaginal walls, no cystocele and no anterior prolapse of the vaginal wall. 49 percent had very little prolapse (grade 1) and 4 percent had prolapse grade 2. Among them, 71 percent had vaginal atrophy as well. Less than 10 percent were being treated with hormone replacement therapy. The majority of them had had two deliveries, and 20 percent were nulliparous (figure 4). Before therapy, 89 percent of the patients had shown severe symptoms of SUI, and 11 percent had shown moderate symptoms. After three FemiLift treatments (fractional pixel CO2 therapy), 40 percent of our patients had no symptoms of SUI anymore , 49 percent
SZD 2/2019
11
CONGRESS-HANDOUT
SGML
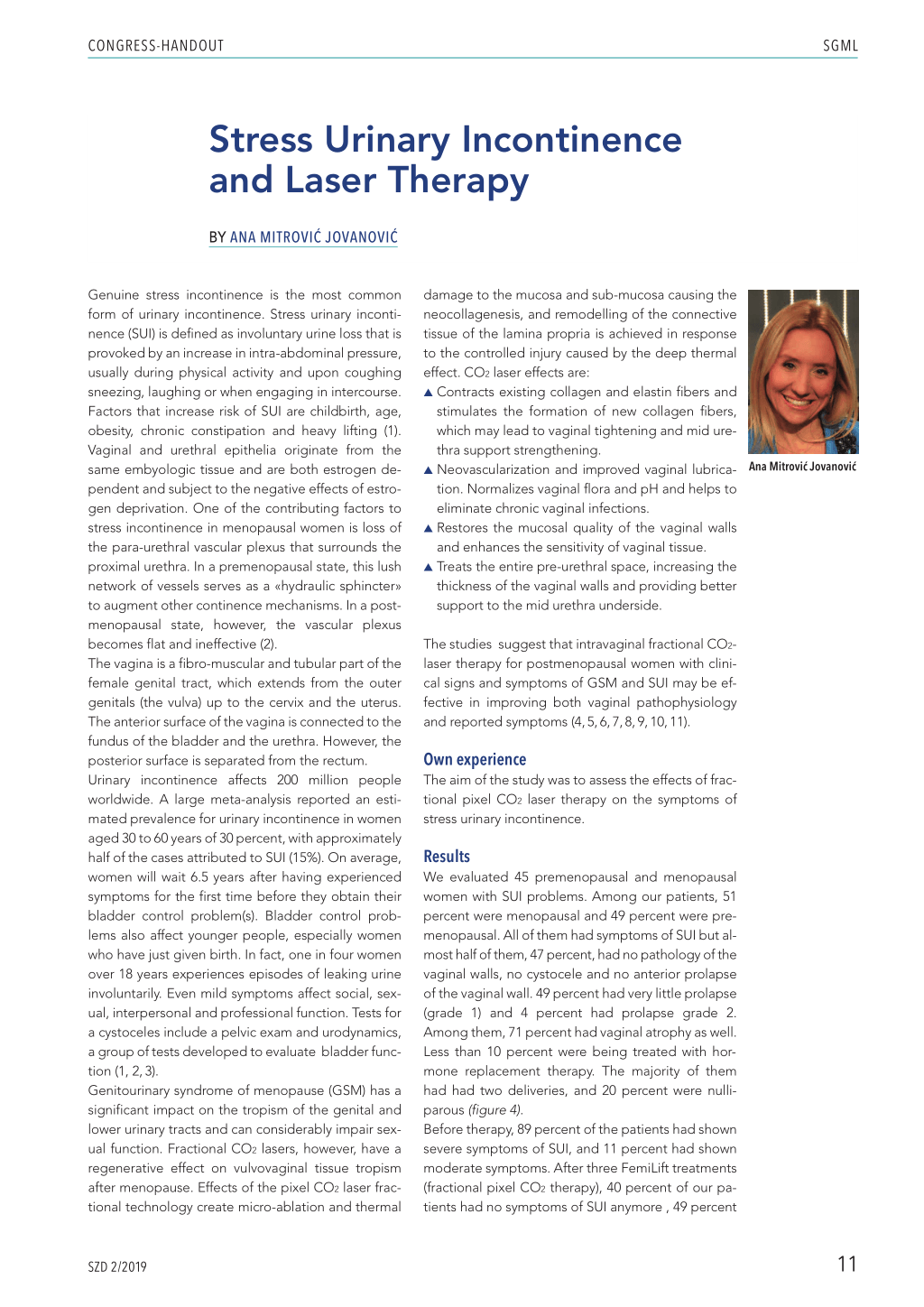
Figure 1 and 2: procedure of vaginal rejuvenation using fractional CO2 laser
Figure 3: vagina and cervix after treatment, showing a normal vaginal discharge, color and quality of the rejuvenation of the vaginal wall
Hormonal TH
Vaginal Atrophy
Menopause
S PAD
Births
Before treatment
Results
Figure 4: Patient characteristics and Results
are very satisfied with the improvement but still occasionally display symptoms, and 11 percent have very mild symptoms of SUI (figure 5). We followed up with our patients and after six months the satisfaction rate was the same as immediately after the third treatment. Moreover, our study on the use of fractional pixel CO2 laser treatment for SUI among premenopausal and menopausal women demonstrated a significant improvement in other parameters such as: L vaginal dryness in 80 percent of cases (32/40) L vaginal itching in 85 percent (34/40) L dyspareunia in 70 percent of cases (28/40) L dysuria in 90 percent (36/40)
L sexual function and overall satisfaction in 95 percent (38/40)
This was tested in a follow-up meeting after 12 weeks. Furthermore, the women reported almost the same satisfaction after 24 and 36 weeks. This results show that we could expect improvement in overall life quality among our patients treated with laser therapy as an additional benefit of the initial treatment of SUI symptoms. Pitsouni furthermore suggests that intravaginal CO2laser therapy for postmenopausal women with clinical signs and symptoms of GSM may be effective in improving both vaginal pathophysiology and reported symptoms (11). Based on data from studies
12 SZD 2/2019
CONGRESS-HANDOUT
lasting up to 1 year, fractional CO2 laser therapy may be an effective and safe treatment for women suffering from symptoms of GSM, although additional studies with larger populations and placebo control are needed to confirm these results (12). Results of Athanasiou study moreover indicate that CO2-laser therapy may contribute to complete regression of dyspareunia and dryness and to reestablishment of normal sexual function in postmenopausal women, in a dose-response manner. An extra fourth or fifth session may further increase the GSM symptom-free rate (13).
Conclusion
The results of laser therapy on urinal incontinence are promising and well accepted by our patients. It has already been shown that laser therapy plays an important therapeutic role in the treatment of several gynecological conditions. Most recently researchers have expressed interest in laser therapy as a non-hormonal treatment for genitourinary syndrome of menopause. Female pelvic floor disorders, such as WA and SUI, remain underdiagnosed and undertreated despite their high frequency and significant impact on quality of life.
These disorders increasing age, but they can be
treated with laser therapy..
L
Correspondence address:
Prof. Dr. Ana Mitrović Jovanović GAK narodni front, Beograd E-Mail: anamitrovicjov@googlemail.com
References 1. Lambrou N et al.: The Jon Hopkins Manual of Gynecology and Obstetrics, Lippin-
cott Williams and Wilkins 199: 216–227. 2. Berec and Novaks: Gynecology. Lippincott Williams and Wilkins 2012. 3. Hampel C et al.: Definition of overactive bladder and epidemiology of urinary
incontinence. Urology 1997; 50: 4–14. 4. https://www.nationalincontinence.com 5. https://www.ics.org 6. Huang LP et al.: Application of fractional laser resurfacing in the treatment of
superficial scar. Chinese journal of plastic surgery 2010; 26(3) :182–185. (engl. Abstract, Artikel auf Chinesisch) 7. Hashim PW et al.: Noninvasive vaginal rejuvenation. Cutis 2018; 102(4): 243–246. 8. Schilling L: Vaginal rejuvenation: whose turf? Med Surg 2018; 37(4): 236–237. 9. Harris V et al.: Vulvo-vaginal rejuvenation: Fact or fiction? Fractional carbon dioxide laser for genitourinary syndrome of menopause., Australas J Dermatol 2018; 59(4): 341–343. 10. Jardin I et al.: CO2 LASER for the treatment of vaginal symptoms of genitourinary syndrome of menopause.Gynecol Obstet Fertil Senol 2018; 46(10-11): 729–734. 11. Pitsouni E et al.: Laser therapy for the genitourinary syndrome of menopause. A systematic review and meta-analysis. Maturitas 2017; 103: 78–88. 12. Sokol ER: Use of a novel fractional CO2 laser for the treatment of genitourinary syndrome of menopause: 1-year outcomes.Menopause. Menopause 2017; 24(7): 810–814. 13. Athanasiou S et al.: CO2-laser for the genitourinary syndrome of menopause.How many laser sessions? Maturitas 2017; 104: 24–28.
SGML