Transkript
CONGRESS HANDOUT
SGML
Use of microwaves for axillary sweat control
Who is not concerned?
BY JOACHIM KRISCHER
Joachim Krischer
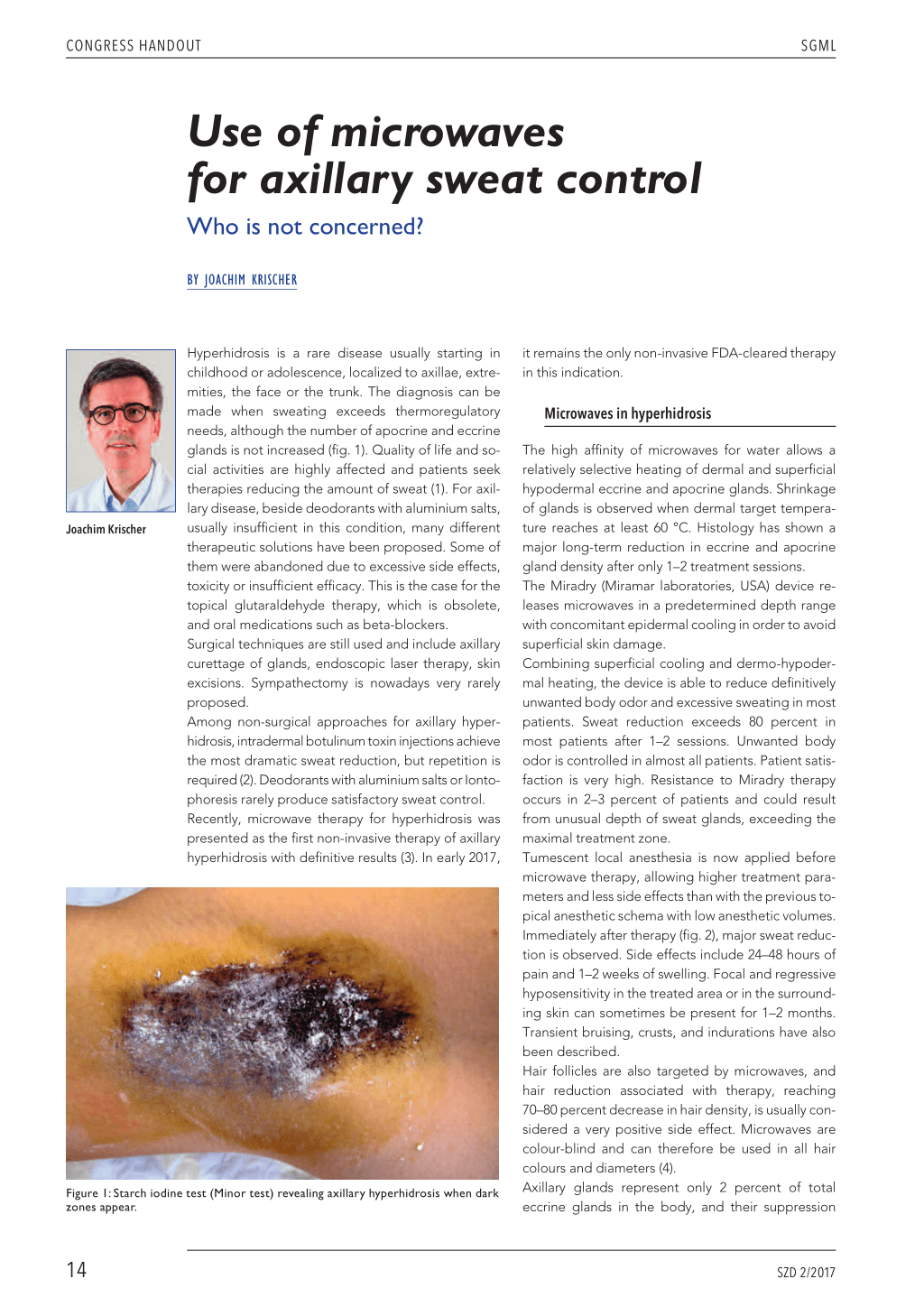
Hyperhidrosis is a rare disease usually starting in childhood or adolescence, localized to axillae, extremities, the face or the trunk. The diagnosis can be made when sweating exceeds thermoregulatory needs, although the number of apocrine and eccrine glands is not increased (fig. 1). Quality of life and social activities are highly affected and patients seek therapies reducing the amount of sweat (1). For axillary disease, beside deodorants with aluminium salts, usually insufficient in this condition, many different therapeutic solutions have been proposed. Some of them were abandoned due to excessive side effects, toxicity or insufficient efficacy. This is the case for the topical glutaraldehyde therapy, which is obsolete, and oral medications such as beta-blockers. Surgical techniques are still used and include axillary curettage of glands, endoscopic laser therapy, skin excisions. Sympathectomy is nowadays very rarely proposed. Among non-surgical approaches for axillary hyperhidrosis, intradermal botulinum toxin injections achieve the most dramatic sweat reduction, but repetition is required (2). Deodorants with aluminium salts or Iontophoresis rarely produce satisfactory sweat control. Recently, microwave therapy for hyperhidrosis was presented as the first non-invasive therapy of axillary hyperhidrosis with definitive results (3). In early 2017,
Figure 1: Starch iodine test (Minor test) revealing axillary hyperhidrosis when dark zones appear.
it remains the only non-invasive FDA-cleared therapy in this indication.
Microwaves in hyperhidrosis
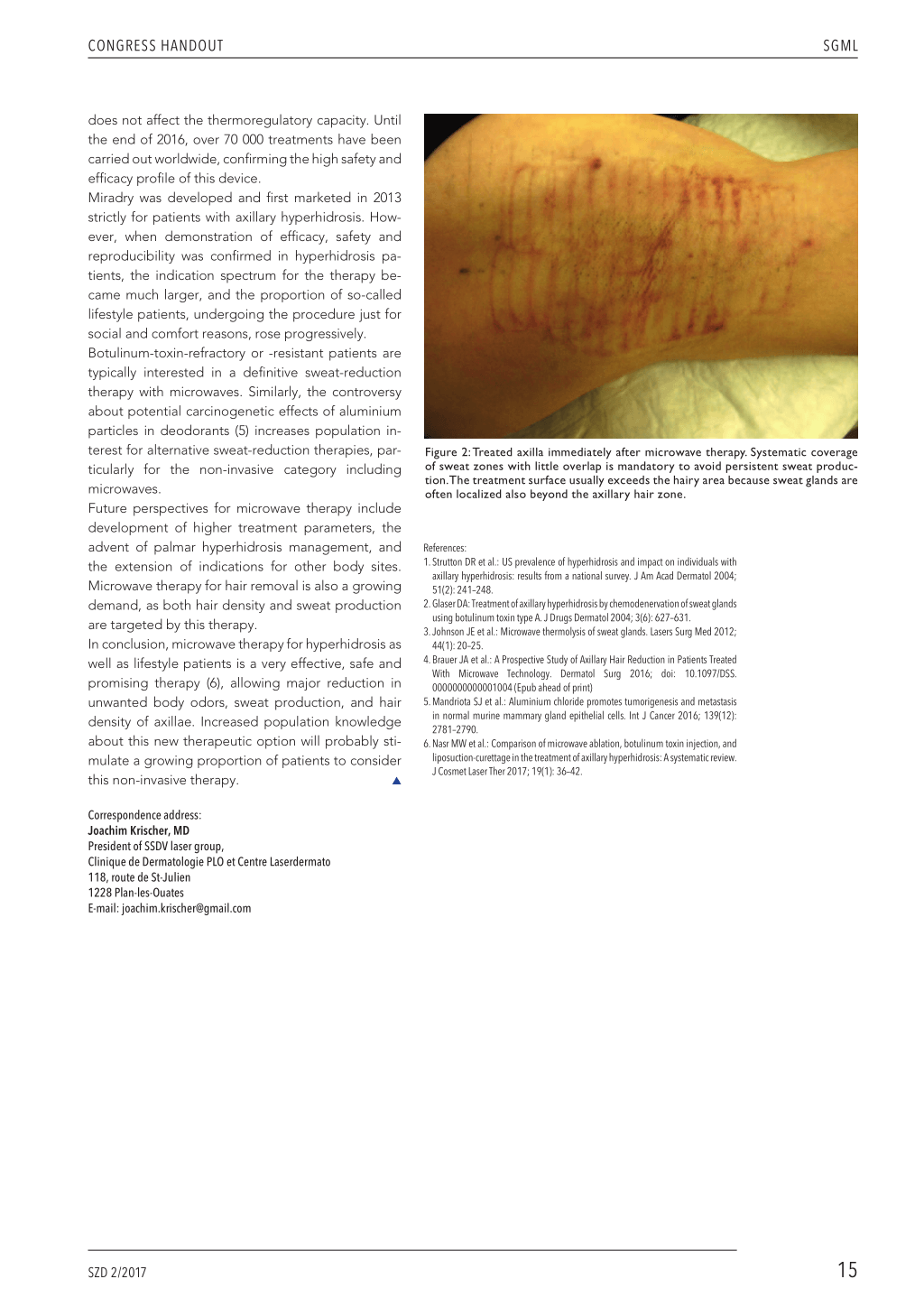
The high affinity of microwaves for water allows a relatively selective heating of dermal and superficial hypodermal eccrine and apocrine glands. Shrinkage of glands is observed when dermal target temperature reaches at least 60 °C. Histology has shown a major long-term reduction in eccrine and apocrine gland density after only 1–2 treatment sessions. The Miradry (Miramar laboratories, USA) device releases microwaves in a predetermined depth range with concomitant epidermal cooling in order to avoid superficial skin damage. Combining superficial cooling and dermo-hypodermal heating, the device is able to reduce definitively unwanted body odor and excessive sweating in most patients. Sweat reduction exceeds 80 percent in most patients after 1–2 sessions. Unwanted body odor is controlled in almost all patients. Patient satisfaction is very high. Resistance to Miradry therapy occurs in 2–3 percent of patients and could result from unusual depth of sweat glands, exceeding the maximal treatment zone. Tumescent local anesthesia is now applied before microwave therapy, allowing higher treatment parameters and less side effects than with the previous topical anesthetic schema with low anesthetic volumes. Immediately after therapy (fig. 2), major sweat reduction is observed. Side effects include 24–48 hours of pain and 1–2 weeks of swelling. Focal and regressive hyposensitivity in the treated area or in the surrounding skin can sometimes be present for 1–2 months. Transient bruising, crusts, and indurations have also been described. Hair follicles are also targeted by microwaves, and hair reduction associated with therapy, reaching 70–80 percent decrease in hair density, is usually considered a very positive side effect. Microwaves are colour-blind and can therefore be used in all hair colours and diameters (4). Axillary glands represent only 2 percent of total eccrine glands in the body, and their suppression
14 SZD 2/2017
CONGRESS HANDOUT
SGML
does not affect the thermoregulatory capacity. Until
the end of 2016, over 70 000 treatments have been
carried out worldwide, confirming the high safety and
efficacy profile of this device.
Miradry was developed and first marketed in 2013
strictly for patients with axillary hyperhidrosis. How-
ever, when demonstration of efficacy, safety and
reproducibility was confirmed in hyperhidrosis pa-
tients, the indication spectrum for the therapy be-
came much larger, and the proportion of so-called
lifestyle patients, undergoing the procedure just for
social and comfort reasons, rose progressively.
Botulinum-toxin-refractory or -resistant patients are
typically interested in a definitive sweat-reduction
therapy with microwaves. Similarly, the controversy
about potential carcinogenetic effects of aluminium
particles in deodorants (5) increases population in-
terest for alternative sweat-reduction therapies, par-
ticularly for the non-invasive category including
microwaves.
Future perspectives for microwave therapy include
development of higher treatment parameters, the
advent of palmar hyperhidrosis management, and
the extension of indications for other body sites.
Microwave therapy for hair removal is also a growing
demand, as both hair density and sweat production
are targeted by this therapy.
In conclusion, microwave therapy for hyperhidrosis as
well as lifestyle patients is a very effective, safe and
promising therapy (6), allowing major reduction in
unwanted body odors, sweat production, and hair
density of axillae. Increased population knowledge
about this new therapeutic option will probably sti-
mulate a growing proportion of patients to consider
this non-invasive therapy.
L
Figure 2: Treated axilla immediately after microwave therapy. Systematic coverage of sweat zones with little overlap is mandatory to avoid persistent sweat production.The treatment surface usually exceeds the hairy area because sweat glands are often localized also beyond the axillary hair zone.
References: 1. Strutton DR et al.: US prevalence of hyperhidrosis and impact on individuals with
axillary hyperhidrosis: results from a national survey. J Am Acad Dermatol 2004; 51(2): 241–248. 2. Glaser DA: Treatment of axillary hyperhidrosis by chemodenervation of sweat glands using botulinum toxin type A. J Drugs Dermatol 2004; 3(6): 627–631. 3. Johnson JE et al.: Microwave thermolysis of sweat glands. Lasers Surg Med 2012; 44(1): 20–25. 4. Brauer JA et al.: A Prospective Study of Axillary Hair Reduction in Patients Treated With Microwave Technology. Dermatol Surg 2016; doi: 10.1097/DSS. 0000000000001004 (Epub ahead of print) 5. Mandriota SJ et al.: Aluminium chloride promotes tumorigenesis and metastasis in normal murine mammary gland epithelial cells. Int J Cancer 2016; 139(12): 2781–2790. 6. Nasr MW et al.: Comparison of microwave ablation, botulinum toxin injection, and liposuction-curettage in the treatment of axillary hyperhidrosis: A systematic review. J Cosmet Laser Ther 2017; 19(1): 36–42.
Correspondence address: Joachim Krischer, MD President of SSDV laser group, Clinique de Dermatologie PLO et Centre Laserdermato 118, route de St-Julien 1228 Plan-les-Ouates E-mail: joachim.krischer@gmail.com
SZD 2/2017
15