Transkript
CONGRESS HANDOUT
SGML
Fractional vs Non-Fractional Laser
Where Are We and Where Are We Going?
There is no doubt that laser resurfacing technologies have revolutionized the treatment of skin tone, texture and pigmentation. Although laser repaving techniques cannot replace a facelift or blepharoplasty, it is clear that the appropriate technology can improve the appearance of lentigines and rhytides, reduce photoaging, improve acne scarring and other forms of dyspigmentation.
Clifford Albert
6
BY CLIFFORD ALBERT
Ablative lasers vaporize tissue layers whereas nonablative lasers are gentler and leave the skin intact. Non fractionated lasers act on the entire treated surface whereas fractionated lasers treat only portions of the treatment area in a pixellated fashion. The fractionated devices produce small columns of thermal injury known as microthermal zones (MTZs) which can be either non-ablative dermal injuries only or both epidermal and dermal injuries with the ablative lasers. Following laser treatment, the skin undergoes a rapid repair process in which the degenerated dermal debris is delivered as columns to the epidermis known as microscopic epidermal necrotic debris (MEND). This rapid healing process is made possible through the surrounding untreated skin. Although it is clear that ablative lasers result in more downtime for the patient they remain the lasers that produce the most dramatic outcomes. Ablative lasers still remain the gold standard for treating the most severe forms of wrinkling, dyspigmentation and scarring. Fractionation distributes the effects of the laser, which increases the number of treatments while minimizing patient downtime and complications. For those patients who seek to avoid the possible side effects of ablative lasers and who accept more moderate results, non-ablative lasers represent an acceptable alternative. While leaving the skin layers intact, non-ablative techniques reduce fine lines, improve skin texture and dyspigmentation. Although the treatments are gentler and require less downtime, they produce a more moderate improvement and require more sessions.
Theory of Selective PhotoThermolysis
To thoroughly understand the principle of laser-tissue interaction, it is important to refer to the theory of Selective PhotoThermolysis (Anderson et al 1983),
which guides the clinician in the safe and effective targeting of chromophores in the skin. The three chromophores in the skin (hemoglobin, water, melanin) may be selectively targeted due to each chromophore’s affinity to absorb a distinct wavelength of light. The target is destroyed when a specific wavelength of sufficient energy is absorbed by the chromophore. In order to avoid collateral photothermal destruction, the pulse width of a given laser must be shorter than the Thermal Relaxation Time of its intended target.
Era of ablative Lasers
During the late 1990s and early 2000s, the gold standard for the treatment of rhytides, dyspigmentation, acne and traumatic scars was the CO2 laser with its tremendous affinity for water. This laser superheats water molecules, and as the water turns into gas, the skin cells are vaporized. This laser was able to remove the entire epidermis and the resultant wound healing cascade would lead to dramatic fibroplasia and neocollagenesis. Typically, downtime lasted between 7–10 days and adverse effects included pain, edema, erythema, infections, hyper- or hypopigmentation which could be permanent. It is clear that the amount of injury is also correlated with the amount of wrinkle reduction. The Er:YAG (2940nm) was introduced as a «gentler» ablative laser and was not supposed to produce the same adverse events as the CO2 laser. Downtimes typically ranged from 5–7 days and could still result in post-laser hypopigmentation. Although the most recent generation of fractionated ablative lasers have reduced the downtime while still allowing effective resurfacing being much safer, they still retain a higher risk of scarring, discoloration and infections of the skin than non-ablative techniques.
SZD 2/2017
CONGRESS HANDOUT
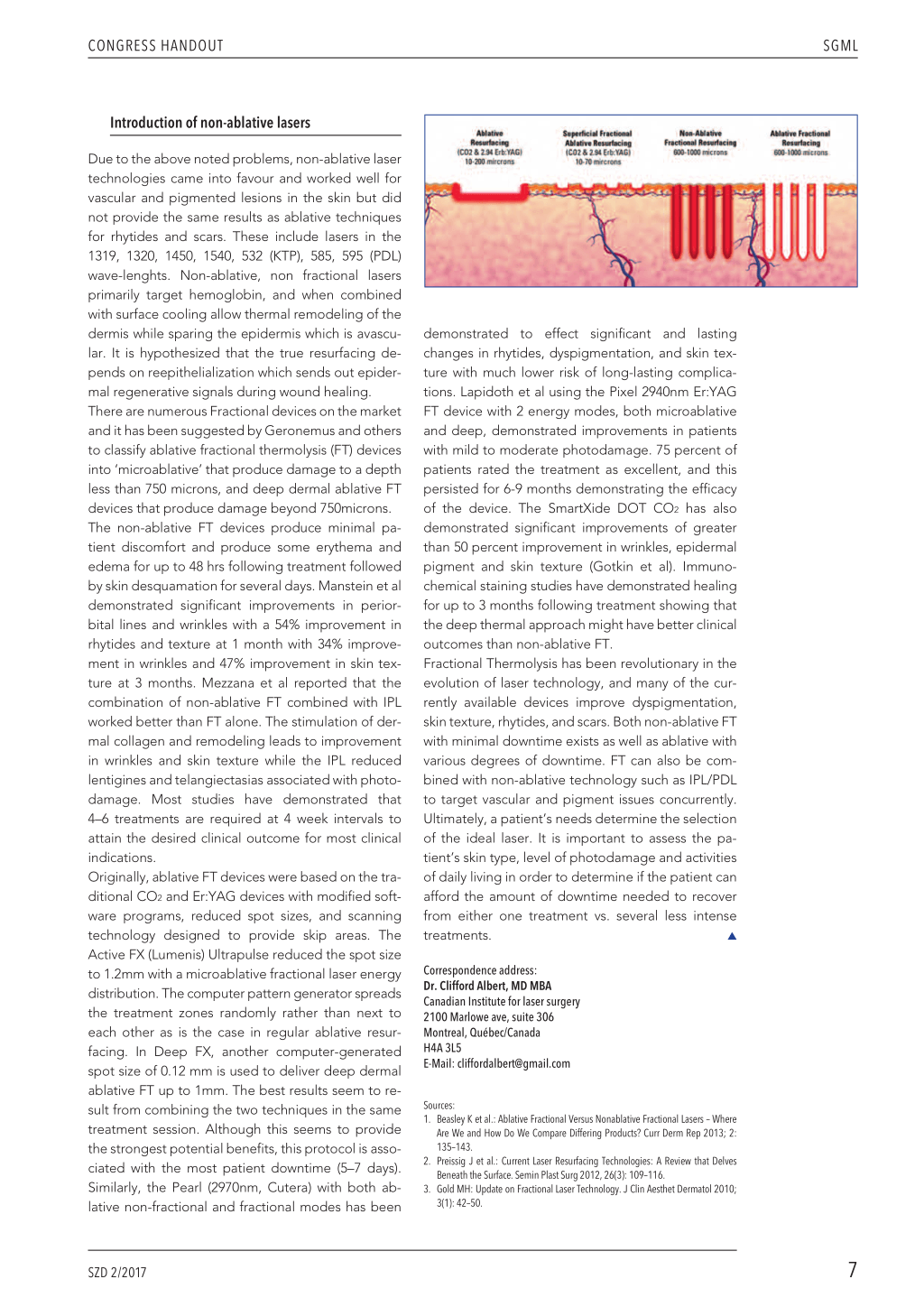
Introduction of non-ablative lasers
Due to the above noted problems, non-ablative laser technologies came into favour and worked well for vascular and pigmented lesions in the skin but did not provide the same results as ablative techniques for rhytides and scars. These include lasers in the 1319, 1320, 1450, 1540, 532 (KTP), 585, 595 (PDL) wave-lenghts. Non-ablative, non fractional lasers primarily target hemoglobin, and when combined with surface cooling allow thermal remodeling of the dermis while sparing the epidermis which is avascular. It is hypothesized that the true resurfacing depends on reepithelialization which sends out epidermal regenerative signals during wound healing. There are numerous Fractional devices on the market and it has been suggested by Geronemus and others to classify ablative fractional thermolysis (FT) devices into ‘microablative’ that produce damage to a depth less than 750 microns, and deep dermal ablative FT devices that produce damage beyond 750microns. The non-ablative FT devices produce minimal patient discomfort and produce some erythema and edema for up to 48 hrs following treatment followed by skin desquamation for several days. Manstein et al demonstrated significant improvements in periorbital lines and wrinkles with a 54% improvement in rhytides and texture at 1 month with 34% improvement in wrinkles and 47% improvement in skin texture at 3 months. Mezzana et al reported that the combination of non-ablative FT combined with IPL worked better than FT alone. The stimulation of dermal collagen and remodeling leads to improvement in wrinkles and skin texture while the IPL reduced lentigines and telangiectasias associated with photodamage. Most studies have demonstrated that 4–6 treatments are required at 4 week intervals to attain the desired clinical outcome for most clinical indications. Originally, ablative FT devices were based on the traditional CO2 and Er:YAG devices with modified software programs, reduced spot sizes, and scanning technology designed to provide skip areas. The Active FX (Lumenis) Ultrapulse reduced the spot size to 1.2mm with a microablative fractional laser energy distribution. The computer pattern generator spreads the treatment zones randomly rather than next to each other as is the case in regular ablative resurfacing. In Deep FX, another computer-generated spot size of 0.12 mm is used to deliver deep dermal ablative FT up to 1mm. The best results seem to result from combining the two techniques in the same treatment session. Although this seems to provide the strongest potential benefits, this protocol is associated with the most patient downtime (5–7 days). Similarly, the Pearl (2970nm, Cutera) with both ablative non-fractional and fractional modes has been
demonstrated to effect significant and lasting
changes in rhytides, dyspigmentation, and skin tex-
ture with much lower risk of long-lasting complica-
tions. Lapidoth et al using the Pixel 2940nm Er:YAG
FT device with 2 energy modes, both microablative
and deep, demonstrated improvements in patients
with mild to moderate photodamage. 75 percent of
patients rated the treatment as excellent, and this
persisted for 6-9 months demonstrating the efficacy
of the device. The SmartXide DOT CO2 has also
demonstrated significant improvements of greater
than 50 percent improvement in wrinkles, epidermal
pigment and skin texture (Gotkin et al). Immuno-
chemical staining studies have demonstrated healing
for up to 3 months following treatment showing that
the deep thermal approach might have better clinical
outcomes than non-ablative FT.
Fractional Thermolysis has been revolutionary in the
evolution of laser technology, and many of the cur-
rently available devices improve dyspigmentation,
skin texture, rhytides, and scars. Both non-ablative FT
with minimal downtime exists as well as ablative with
various degrees of downtime. FT can also be com-
bined with non-ablative technology such as IPL/PDL
to target vascular and pigment issues concurrently.
Ultimately, a patient’s needs determine the selection
of the ideal laser. It is important to assess the pa-
tient’s skin type, level of photodamage and activities
of daily living in order to determine if the patient can
afford the amount of downtime needed to recover
from either one treatment vs. several less intense
treatments.
L
Correspondence address: Dr. Clifford Albert, MD MBA Canadian Institute for laser surgery 2100 Marlowe ave, suite 306 Montreal, Québec/Canada H4A 3L5 E-Mail: cliffordalbert@gmail.com
Sources: 1. Beasley K et al.: Ablative Fractional Versus Nonablative Fractional Lasers – Where
Are We and How Do We Compare Differing Products? Curr Derm Rep 2013; 2: 135–143. 2. Preissig J et al.: Current Laser Resurfacing Technologies: A Review that Delves Beneath the Surface. Semin Plast Surg 2012, 26(3): 109–116. 3. Gold MH: Update on Fractional Laser Technology. J Clin Aesthet Dermatol 2010; 3(1): 42–50.
SZD 2/2017
SGML
7